

Pediatric subcutaneous nasal glial heterotopia
- PMID: 39926455
- PMCID: PMC11799680
- DOI: 10.25259/SNI_93_2024
Pediatric subcutaneous nasal glial heterotopia
Abstract
Background: Nasal glial heterotopias (NGHs) are benign lesions diagnosed at birth that are treated with complete surgical excision and have a low recurrence rate. The impact of the timing of resection on the patients' outcome remains unclear.
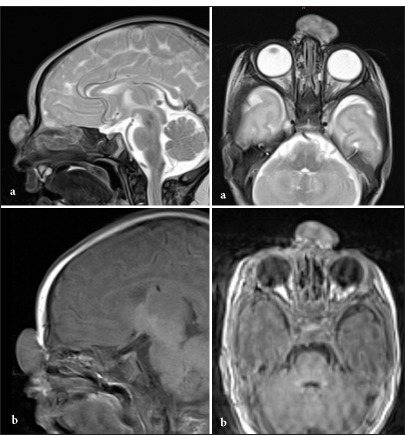
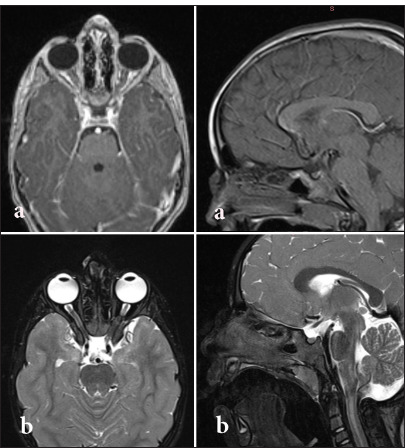
Case description: We report a case of pediatric midline subcutaneous extranasal glial heterotopia over the nasal bridge in a 4-day-old female newborn. At the age of 6 months, she underwent a complete surgical excision. Follow-up magnetic resonance imaging at 3 years showed no evidence of recurrence. A summary of the 19 published cases of the specific entity of purely subcutaneous extranasal glial heterotopia among the pediatrics age group in the literature is presented, and the timing of surgery in relation to outcome is discussed.
Conclusion: Our review revealed that surgery for NGH can be safely performed when the child is 6-12 months old, and the child should be followed probably until school age.
Keywords: Nasal cerebral heterotopia; Nasal glial heterotopia; Nasal glioma; Neuroglial heterotopia.
Copyright: © 2025 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures


Similar articles
-
Histopathologic features of nasal glial heterotopia (nasal glioma).Childs Nerv Syst. 2022 Jan;38(1):63-75. doi: 10.1007/s00381-021-05369-4. Epub 2021 Sep 25. Childs Nerv Syst. 2022. PMID: 34562130
-
Unveiling Nasal Glial Heterotopia: A Pathological Perspective.Cureus. 2024 Apr 30;16(4):e59341. doi: 10.7759/cureus.59341. eCollection 2024 Apr. Cureus. 2024. PMID: 38817464 Free PMC article.
-
Nasal glial heterotopia: a clinicopathologic and immunophenotypic analysis of 10 cases with a review of the literature.Ann Diagn Pathol. 2003 Dec;7(6):354-9. doi: 10.1016/j.anndiagpath.2003.09.010. Ann Diagn Pathol. 2003. PMID: 15018118 Review.
-
A CARE-compliant article: Extranasal glial heterotopia in a female infant: A case report.Medicine (Baltimore). 2018 Sep;97(38):e12000. doi: 10.1097/MD.0000000000012000. Medicine (Baltimore). 2018. PMID: 30235657 Free PMC article.
-
Parapharyngeal Neuroglial Heterotopia: A Case Report and Literature Review.Am J Case Rep. 2020 Nov 6;21:e926300. doi: 10.12659/AJCR.926300. Am J Case Rep. 2020. PMID: 33156818 Free PMC article. Review.
References
-
- Amanullah MM, Moazam F, Attar Z. The extranasal glioma-a cause of neonatal respiratory distress. J Pak Med Assoc. 1996;46:61–2. - PubMed
-
- Bajaj MS, Kashyap S, Wagh VB, Pathak H, Shrey D. Glial heterotopia of the orbit and extranasal region: An unusual entity. Clin Exp Ophthalmol. 2005;33:513–5. - PubMed
-
- Charles NC, Lisman RD, Patel P, Callahan AB. Nasal glioma: A rare cause of congenital inner canthal swelling. Ophthal Plast Reconstr Surg. 2018;34:e93–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources