

Incidence, Risk Factors, and Outcomes of Recurrent Laryngeal Nerve Injury and Dysphonia Following Anterior Cervical Spine Surgery: A Systematic Review and Meta-Analysis
- PMID: 39926627
- PMCID: PMC11807342
- DOI: 10.7759/cureus.78763
Incidence, Risk Factors, and Outcomes of Recurrent Laryngeal Nerve Injury and Dysphonia Following Anterior Cervical Spine Surgery: A Systematic Review and Meta-Analysis
Abstract
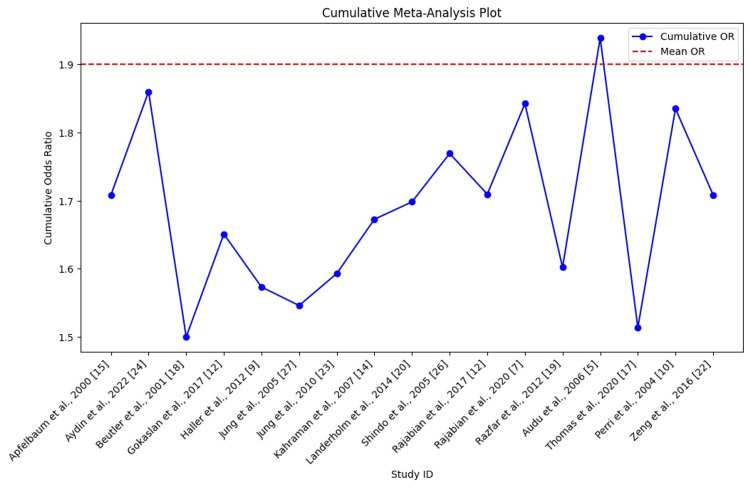
Anterior cervical spine surgery (ACSS) is an effective treatment for various cervical spine conditions but carries a risk of recurrent laryngeal nerve (RLN) injury and dysphonia. This systematic review and meta-analysis aimed to evaluate the incidence of these complications and their associated risk factors. An analysis of 17 studies involving 5,706 patients revealed a pooled RLN injury incidence of 3.41% and a dysphonia incidence of 2.5%. Prolonged surgeries exceeding two hours and multilevel procedures were associated with higher risks, while implant material demonstrated minimal impact. These findings highlight the importance of surgical planning to mitigate RLN injury risk and improve patient outcomes in ACSS.
Keywords: anterior cervical spine surgery; dysphonia; implant materials; recurrent laryngeal nerve injury; surgical risk factors.
Copyright © 2025, Abu-Gameh et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures




References
-
- What's new in spine surgery. Bridwell KH, Anderson PA, Boden SD, Vaccaro AR, Wang JC. J Bone Joint Surg Am. 2009;91:1822–1834. - PubMed
-
- Recurrent laryngeal nerve injury after thyroid surgery: an analysis of 11,370 patients. Gunn A, Oyekunle T, Stang M, Kazaure H, Scheri R. J Surg Res. 2020;255:42–49. - PubMed
-
- The role of peripheral nerve surgery in the treatment of chronic pain associated with amputation stumps. Ducic I, Mesbahi AN, Attinger CE, Graw K. Plast Reconstr Surg. 2008;121:908–914. - PubMed
-
- Recurrent laryngeal nerve palsy after anterior cervical spine surgery: the impact of endotracheal tube cuff deflation, reinflation, and pressure adjustment. Audu P, Artz G, Scheid S, et al. Anesthesiology. 2006;105:898–901. - PubMed
Publication types
LinkOut - more resources
Full Text Sources