

The Global Burden of Cirrhosis and Other Chronic Liver Diseases in 2021
- PMID: 39927433
- PMCID: PMC11808647
- DOI: 10.1111/liv.70001
The Global Burden of Cirrhosis and Other Chronic Liver Diseases in 2021
Abstract
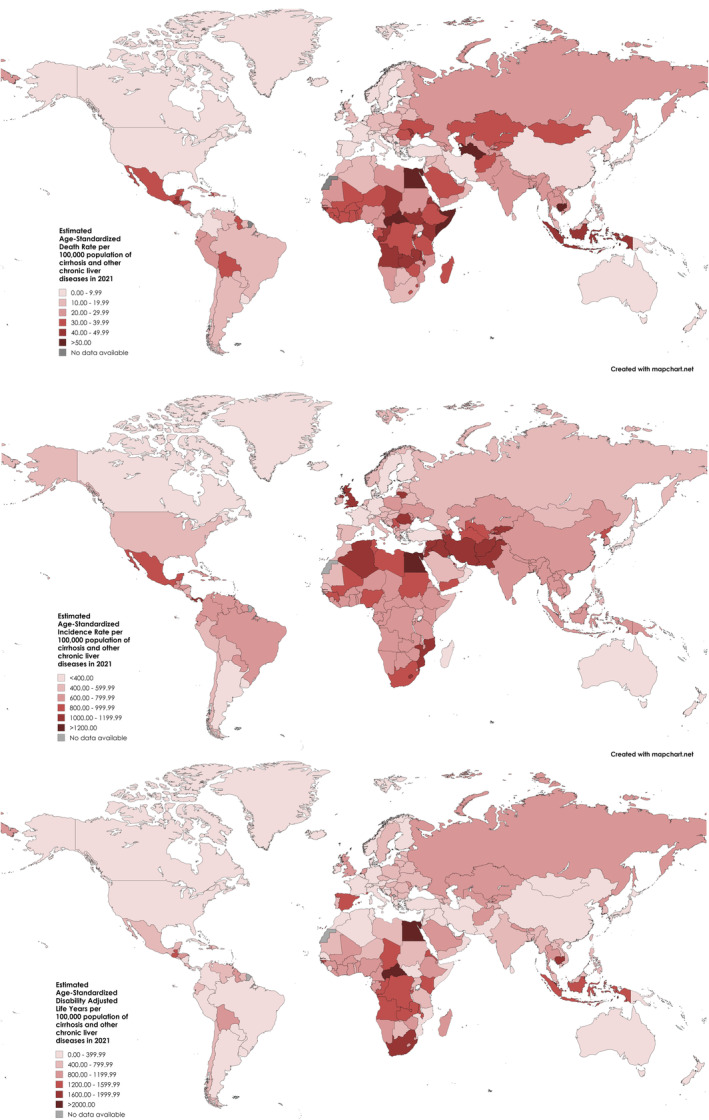
Background and aim: The burden of cirrhosis and other chronic liver diseases has changed in recent years due to shifts in the contributing aetiologies. We estimated the burden of cirrhosis and other chronic liver diseases, including etiological and regional differences, across 204 countries and territories from 2010 to 2021.
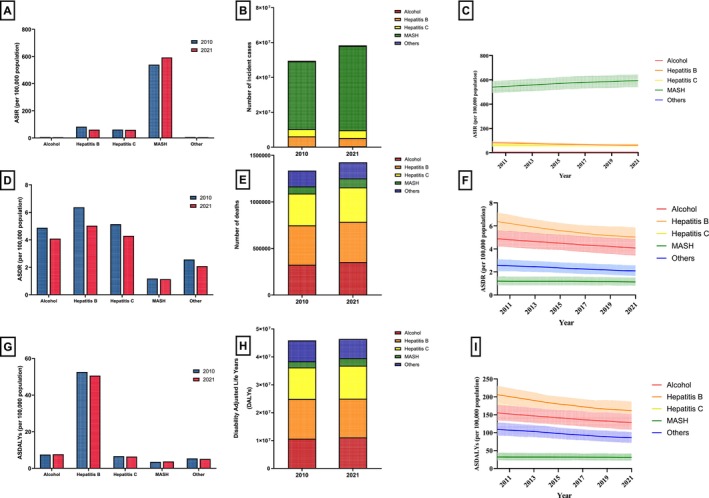
Approach and results: We analysed temporal trends in the burden of cirrhosis and other chronic liver diseases utilising data from the Global Burden of Disease Study 2021. We estimated annual frequencies and age-standardised rates (ASRs) of incident cases, deaths and disability-adjusted life-years (DALYs) by sex, country, World Health Organisation region and its contributing aetiologies. In 2021, there were an estimated 58 417 006 incident cases, 1 425 142 deaths and 46 417 777 DALYs related to cirrhosis and other chronic liver diseases. From 2010 to 2021, there was a rise in age-standardised incidence rates (ASIRs) (APC: +0.35%) but age-standardised death rates (ASDRs) (APC: -1.74%) and age-standardised disability-adjusted life-years (ASDALYs) (APC: -1.85%) declined. Cirrhosis related to metabolic dysfunction-associated steatohepatitis (MASH) contributed to 48 310 981 incident cases in 2021 and was largely responsible for the overall increase in ASIRs from 2010 to 2021. Cirrhosis and other chronic liver diseases related to MASH were the only aetiology with a rise in ASIR (APC: +0.86%). Age-standardised deaths related to all aetiologies of cirrhosis and other chronic liver diseases declined during the study period. Age-standardised deaths and DALYs related to MASH increased in the Americas, unlike all other world regions where they declined or remained stable.
Conclusions: Age-adjusted deaths related to cirrhosis and other chronic liver diseases are declining. However, the age-adjusted incidence of cirrhosis and other chronic liver diseases is increasing, driven by increases in the incidence of MASH.
Keywords: chronic liver disease; cirrhosis; global burden.
© 2025 The Author(s). Liver International published by John Wiley & Sons Ltd.
Conflict of interest statement
C.H.N. has served as a consultant for Boxer Capital. R.L. serves as a consultant to Aardvark Therapeutics, Altimmune, Anylam/Regeneron, Amgen, Arrowhead Pharmaceuticals, AstraZeneca, Bristol‐Myer Squibb, CohBar, Eli Lilly, Galmed, Gilead, Glympse Bio, Hightide, Inipharma, Intercept, Inventiva, Ionis, Janssen Inc., Madrigal, Metacrine Inc., NGM Biopharmaceuticals, Novartis, Novo Nordisk, Merck, Pfizer, Sagimet, Theratechnologies, 89 bio, Terns Pharmaceuticals and Viking Therapeutics. In addition, his institutions received research grants from Arrowhead Pharmaceuticals, Astrazeneca, Boehringer‐Ingelheim, Bristol‐Myers Squibb, Eli Lilly, Galectin Therapeutics, Galmed Pharmaceuticals, Gilead, Intercept, Hanmi, Intercept, Inventiva, Ionis, Janssen, Madrigal Pharmaceuticals, Merck, NGM Biopharmaceuticals, Novo Nordisk, Merck, Pfizer, Sonic Incytes and Terns Pharmaceuticals. D.H., co‐founder of LipoNexus Inc., has served as an advisory board member for Gilead. All other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures





References
-
- Smith A., Baumgartner K., and Bositis C., “Cirrhosis: Diagnosis and Management,” American Family Physician 100, no. 12 (2019): 759–770. - PubMed
-
- World Health Organization , Global Hepatitis Report 2024: Action for Access in Low‐ and Middle‐Income Countries (World Health Organization, 2024).
