

Impact of cerebrospinal fluid leukocyte infiltration and activated neuroimmune mediators on survival with HIV-associated cryptococcal meningitis
- PMID: 39928682
- PMCID: PMC11844869
- DOI: 10.1371/journal.pntd.0012873
Impact of cerebrospinal fluid leukocyte infiltration and activated neuroimmune mediators on survival with HIV-associated cryptococcal meningitis
Abstract
Introduction: Cryptococcal meningitis remains a prominent cause of death in persons with advanced HIV disease. CSF leukocyte infiltration predicts survival at 18 weeks; however, how CSF immune response relates to CSF leukocyte infiltration is unknown.
Methods: We enrolled 401 adults with HIV-associated cryptococcal meningitis in Uganda who received amphotericin and fluconazole induction therapy. We assessed the association of CSF leukocytes, chemokine, and cytokine responses with 18-week survival.
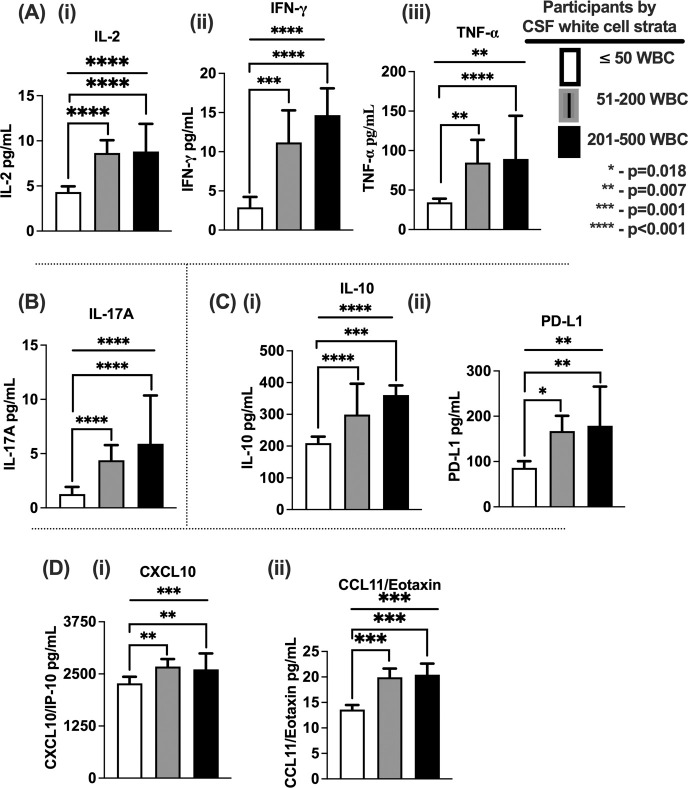
Results: Participants with CSF leukocytes ≥50/microliter had a higher probability of 18-week survival compared with those with ≤50 cells/microliter (68% (52/77 vs. 52% (151/292); Hazard Ratio = 1.63, 95% confidence interval 1.14-2.23; p = 0.008). Survival was also associated with higher expression of T helper (Th)-1, Th17 cytokines, and immune regulatory elements. CSF levels of Programmed Death-1 Ligand, CXCL10, and Interleukin (IL)-2 independently predicted survival. In multivariate analysis, CSF leukocytes were inversely associated with CSF fungal burden and positively associated with CSF protein and immune parameters (interferon-gamma (IFN-γ), IL-17A, tumor necrosis factor alpha (TNF)-α, and circulating CD4+ and CD8+ T cells).
Conclusion: 18-week survival after diagnosis of cryptococcal meningitis was associated with higher CSF leukocytes at baseline with greater T helper 1 (IFN-γ, IL-2 and TNF-α cytokines), T helper 17 (IL-17A cytokine) and CXCR3+ T cell (CXCL10 chemokine) responses. These results highlight the interdependent contribution of soluble and cellular immune responses in predicting survival and may support potential pathways for adjunctive immune therapy in HIV-associated cryptococcal meningitis.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
SO was a Fogarty and GlaxoSmithKline-Trust in Science Africa funded doctoral scholar at Infectious Diseases Institute, Makerere University. Part of the work contributed to the doctoral thesis defended at the Makerere University and cited in this article on reference 40. AMK was a member of a study data safety monitoring board.
Figures



Update of
-
Impact of Cerebrospinal Fluid Leukocyte Infiltration and Neuroimmmune Mediators on Survival with HIV-Associated Cryptococcal Meningitis.medRxiv [Preprint]. 2024 May 31:2024.05.29.24308130. doi: 10.1101/2024.05.29.24308130. medRxiv. 2024. Update in: PLoS Negl Trop Dis. 2025 Feb 10;19(2):e0012873. doi: 10.1371/journal.pntd.0012873. PMID: 38854002 Free PMC article. Updated. Preprint.
References
MeSH terms
Substances
Grants and funding
- R01 NS086312/NS/NINDS NIH HHS/United States
- D43 TW009771/TW/FIC NIH HHS/United States
- I01 CX001464/CX/CSRD VA/United States
- K24 AI096925/AI/NIAID NIH HHS/United States
- K24 AI184270/AI/NIAID NIH HHS/United States
- K01 TW010268/TW/FIC NIH HHS/United States
- R21 NS065713/NS/NINDS NIH HHS/United States
- R01 AI078934/AI/NIAID NIH HHS/United States
- T32 AI055433/AI/NIAID NIH HHS/United States
- R25 TW009345/TW/FIC NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- D43 TW009345/TW/FIC NIH HHS/United States
- R01 AI162786/AI/NIAID NIH HHS/United States
- R01 AI108479/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
