

Effect of emergency department opioid prescribing on health outcomes
- PMID: 39929491
- PMCID: PMC11810442
- DOI: 10.1503/cmaj.241542
Effect of emergency department opioid prescribing on health outcomes
Abstract
Background: The relation between emergency department opioid prescribing and subsequent harm is complex and poorly studied. We sought to quantify adverse outcomes, incremental risk, and rates of prolonged opioid use among emergency department patients receiving an opioid prescription and propensity-matched controls.
Methods: We used administrative data to sample all Alberta emergency department visits over 10 years, excluding patients with cancer, palliative care, or concurrent opioid use. Treated patients filled an opioid prescription within 72 hours after their index visit; untreated patients did not. We generated propensity scores to identify matched controls among untreated patients. The 1-year primary composite outcome included opioid-related emergency visits (e.g., overdoses), new opioid agonist therapy, all-cause hospital admission, or death. The secondary outcome was prolonged opioid use.
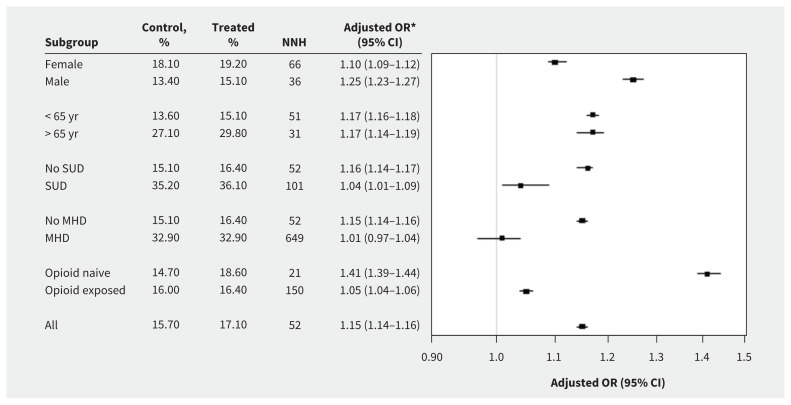
Results: After 13 028 575 eligible visits, 689 074 patients (5.3%) filled an opioid prescription. The mean age was 43.9 years, and 49.8% of patients were female. Most were high-acuity patients with traumatic, gastrointestinal-genitourinary, or musculoskeletal complaints. Patients who received opioids experienced 1.4% more primary outcome events (17.1% v. 15.7%), driven by all-cause hospital admissions (16.4% v. 15.1%; number needed to harm [NNH] = 53) and prolonged opioid use (4.5% v. 3.3%; NNH = 59). Opioid-related visits, new opioid agonist treatment, and mortality were unaffected. Incremental risk was low for patients with documented mental health conditions or substance use, and was highest for opioid-naive patients, older patients, and males.
Interpretation: Emergency department opioid prescriptions were associated with small increases in subsequent opioid prescription use and hospital admission, particularly in older and opioid-naive patients, and males; they were not associated with overdoses, new opioid agonist therapy, or mortality. Physicians should understand patient-specific incremental risks when prescribing opioids for acute pain.
© 2025 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests:: Jake Hayward reports funding from the Canadian Institutes of Health Research (CIHR) and the Canadian Association of Emergency Physicians. Rhonda Rosychuk declares a project grant from CIHR. Andrew McRae reports project grants from CIHR and unrestricted research funding from Roche Diagnostics Canada for unrelated research work. Aynharan Sinnarajah reports grant funding from CIHR and logistical support from Alberta Health Services (AHS). Robert Tanguay is director of the Canadian Academy for Addiction Psychiatry and co-chair of the Alberta Pain Strategy; he also declares roles with the Canadian Addiction Council, Calgary Police Comission, Alberta Association of Police Governance, Alberta Clinical Code Review Board, Queen’s University Ignite Conference, Canadian Society of Addiction Medicine Policy Committee, and Pain Society of Alberta. He has received lecture honoraria from the Master Clinician Alliance and Indivior Canada, and declares travel honoraria from International Foundation of Employee Benefit Plans. Dr. Tanguay declares stock with Newly Institute; Telus; Apple; Becton, Dickinson and Company; Numinus Wellness; and Mind Medicine. Kathryn Dong has received lecture honoraria from the Alberta Society for Human Toxicology and travel support from the Royal College of Physicians and Surgeons of Canada to attend meetings in her role as the chair of the Area of Focused Competence Committee in Addiction Medicine. As Alberta Health Services Chair in Emergency Medicine Research, Dr. Dong reports salary support, paid via the University of Alberta. Lori Montgomery reports funding for a pilot clinical trial of a medication for opioid withdrawal from Hotchkiss Brain Institute (University of Calgary), Alberta Innovates, and teaching honoraria from Alberta College of Family Physicians, University of Calgary, and University of British Columbia. Grant Innes reports support from AHS and CIHR. No other competing interests were declared.
Figures


Comment in
-
Preventing harms from first prescriptions of opioids.CMAJ. 2025 Feb 9;197(5):E133-E134. doi: 10.1503/cmaj.250094. CMAJ. 2025. PMID: 39929493 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources