

Sex and outcomes of patients with microsatellite instability-high and BRAF V600E mutated metastatic colorectal cancer receiving immune checkpoint inhibitors
- PMID: 39929672
- PMCID: PMC11815414
- DOI: 10.1136/jitc-2024-010598
Sex and outcomes of patients with microsatellite instability-high and BRAF V600E mutated metastatic colorectal cancer receiving immune checkpoint inhibitors
Abstract
Background: Immune checkpoint inhibitors (ICIs) are the gold standard therapy in patients with deficient mismatch repair (dMMR)/microsatellite instability-high (MSI-H) metastatic colorectal cancer (mCRC). A significant proportion of patients show resistance, making the identification of determinants of response crucial. Growing evidence supports the role of sex in determining susceptibility to anticancer therapies, but data is lacking for patients with MSI-H CRC.
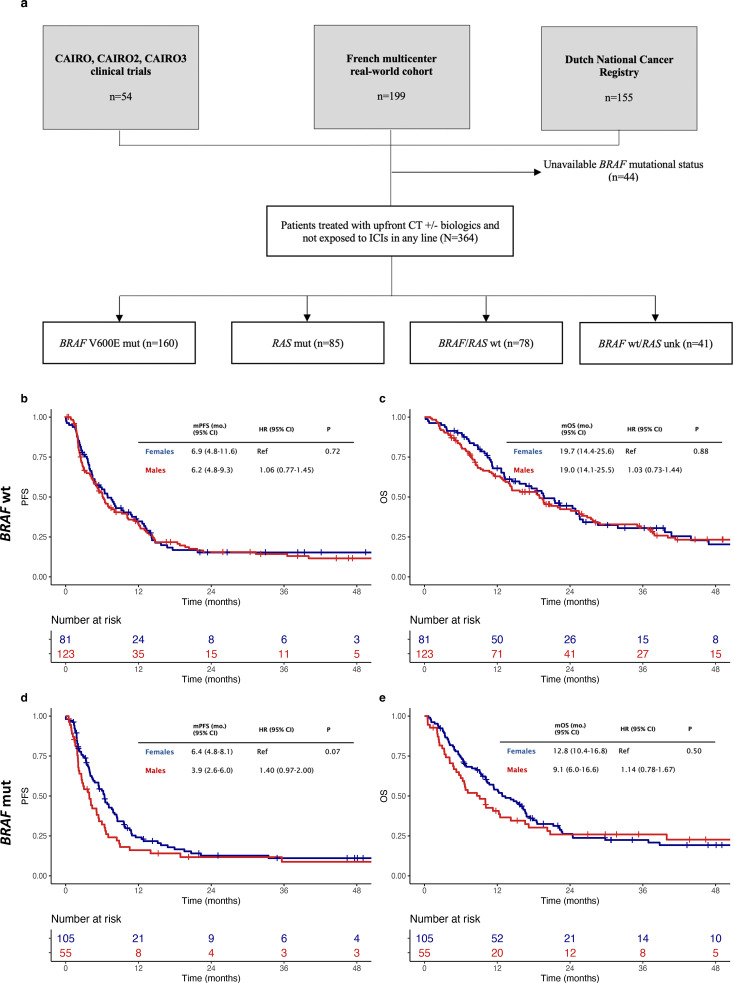
Methods: In this real-world cohort comprising 624 patients with MSI-H mCRC receiving ICIs, we investigated the impact of sex on patients' outcomes, overall and according to RAS-BRAF mutational status or type of treatment (anti-PD-(L)1 with or without anti-CTLA-4 agents). We then investigated these associations also in two independent cohorts of patients with early-stage or advanced MSI-H CRC unexposed to ICIs. Finally, we explored two public microarray and RNA-seq datasets from patients with non-metastatic or metastatic MSI-H CRC to gain translational insights on the association between sex, BRAF status and immune contextures/ICI efficacy.
Results: Although no differences were observed between females and males either overall or in the BRAF wild-type cohort, male sex was associated with inferior progression-free survival (PFS) and overall survival (OS) in the BRAF mutated cohort (in multivariable models, HR for PFS: 1.79, 95% CI: 1.13 to 2.83, p=0.014, and for OS: 2.33, 95% CI: 1.36 to 3.98, p=0.002). Males receiving anti-PD-(L)1 monotherapy had the worst outcomes, with a 3-year PFS and 3-year OS of 23.9% and 41.8%, respectively, while the addition of anti-CTLA-4 agents rescued such a worse outcome. We also observed that females experienced a higher frequency of any-grade immune-related adverse events. Conversely, sex was not prognostic in the independent cohorts of patients with MSI-H CRCs not treated with ICIs. Exploratory transcriptomic analyses suggest that tumors of males with BRAF mutated MSI-H metastatic CRC are characterized by an enrichment of androgen receptor signature and an immune-depleted microenvironment, with a reduction in memory B cells, activated natural killer cells, and activated myeloid dendritic cells.
Conclusions: Overall, our findings suggest a complex interplay between sex and BRAF mutational status that may modulate the activity of ICIs in patients with MSI-H mCRC and pave the way to novel tailored strategies.
Keywords: Colorectal Cancer; Immune Checkpoint Inhibitor; Microsatellite; Mismatch repair - MMR.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: JZ: supported by the National University Health System Seed Fund (NUHSRO/2024/008/RO5+6/Seed-Sep23/01), National University Hospital Junior Research Award 2023 (JRA/Sep23/002), Chan Heng Leong Education & Research Fund 2024 award by the National University Hospital Singapore, 2025 Conquer Cancer Merit Award, and Dean's Research Development Award awarded by the Yong Loo Lin School of Medicine, National University of Singapore.EE: reports roles as consultant/advisor and/or honoraria, travel grants, and research grants from Amgen, Bayer, Hoffman-La Roche, Merck Serono, Sanofi, Pierre Fabre, MSD, Organon, Novartis, and Servier, and reports institutional research funding from Amgen Inc., Array Biopharma Inc., AstraZeneca Pharmaceuticals LP, BeiGene, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Debiopharm International SA, F. Hoffmann-La Roche Ltd., Genentech Inc., HalioDX SAS, Hutchison MediPharma International, Janssen-Cilag SA, MedImmune, Menarini, Merck Health KGAA, Merck Sharp & Dohme, Merus NV, Mirati, Novartis Farmacéutica SA, Pfizer, Pharma Mar, Sanofi Aventis Recherche & Développement, Servier, and Taiho Pharma USA Inc.SL: reports roles as consultant or advisor for Amgen, Astra Zeneca, Bristol-Myers Squibb, Daiichi-Sankyo, Incyte, Lilly, Merck Serono, MSD, Servier, and reports research funding from Amgen, Astellas, Astra-Zeneca, Bayer, BMS Daichii Sankyo, Hutchinson, Incyte, Merck Serono, Mirati, MSD, Pfizer, Roche. She is part of speakers’ bureau of Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Lilly, Merck Serono, Pierre Fabre, Roche, Servier.MJO: reports roles as consultant or advisor for Bristol Myers Squibb, Roche/Genentech, Gritstone Bio, MedImmune, Novartis, Promega, Spectrum Pharmaceuticals, Array BioPharma, Janssen, Pfizer, 3D Medicines, Merck, Eisai, and reports research funding from Bristol Myers Squibb, Merck, Roche, MedImmune.TA: reports attending advisory board meetings and receiving consulting fees from Aptitude heath, AstraZeneca, Astellas, Bristol Myers Squibb, Gritstone Oncology, GamaMabs Pharma Sa, Gilead, GlaxoSmithKline, Merck & Co. Inc., Nordic Oncology, Pierre Fabre, Seagen, Servier and Transgène; honoraria from AstraZeneca, Bristol Myers Squibb, GlaxoSmithKline, Merck & Co. Inc., Pierre Fabre, Roche, Sanofi Seagen and Servier; and support for meetings from Merck & Co. Inc. and Servier.RS: reports attending advisory board meetings for Bristol Myers Squibb, Merck, Eisai, Bayer, Taiho, Novartis, MSD, GSK, DKSH, Astellas, Pierre-Fabre, Tavotek; receiving honoraria for talks from MSD, Eli Lilly, BMS, Roche, Taiho, Astra Zeneca, DKSH, Ipsen, Daiichi Sankyo, Beigene, Astellas; receiving travel support from Roche, Astra Zeneca, Taiho, Eisai, DKSH, Ipsen, receiving research funding from Paxman Coolers, MSD, Natera, CytoMed Therapeutics and has patents pending with Auristone and Paxman.FP: reports receiving Research funding (to Institution) from Lilly, BMS, Incyte, AstraZeneca, Amgen, Agenus, Rottapharm. Personal honoraria as an invited speaker from BeiGene, Daiichi-Sankyo, Seagen, Astellas, Ipsen, AstraZeneca, Servier, Bayer, Takeda, Johnson & Johnson, BMS, MSD, Amgen, Merck-Serono, Pierre-Fabre. Advisory/Consultancy from BMS, MSD, Amgen, Pierre-Fabre, Johnson & Johnson, Servier, Bayer, Takeda, Astellas, GSK, Daiichi-Sankyo, Pfizer, BeiGene, Jazz Pharmaceuticals, Incyte, Rottapharm, Merck-Serono, Italfarmaco, Gilead, AstraZeneca, Agenus.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials