

Effect of early and later prone positioning on outcomes in invasively ventilated COVID-19 patients with acute respiratory distress syndrome: analysis of the prospective COVID-19 critical care consortium cohort study
- PMID: 39930162
- PMCID: PMC11810853
- DOI: 10.1186/s13613-025-01422-6
Effect of early and later prone positioning on outcomes in invasively ventilated COVID-19 patients with acute respiratory distress syndrome: analysis of the prospective COVID-19 critical care consortium cohort study
Erratum in
-
Correction: Effect of early and later prone positioning on outcomes in invasively ventilated COVID-19 patients with acute respiratory distress syndrome: analysis of the prospective COVID-19 critical care consortium cohort study.Ann Intensive Care. 2025 Mar 28;15(1):44. doi: 10.1186/s13613-025-01466-8. Ann Intensive Care. 2025. PMID: 40148711 Free PMC article. No abstract available.
Abstract
Background: Prone positioning of patients with COVID-19 undergoing invasive mechanical ventilation (IMV) is widely used, but evidence of efficacy remains sparse. The COVID-19 Critical Care Consortium has generated one of the largest global datasets on the management and outcomes of critically ill COVID-19 patients. This prospective cohort study investigated the association between prone positioning and mortality and in particular focussed on timing of treatment.
Methods: We investigated the incidence, demographic profile, management and outcomes of proned patients undergoing IMV for COVID-19 in the study. We compared outcomes between patients prone positioned within 48 h of IMV to those (i) never proned, and (ii) proned only after 48 h.
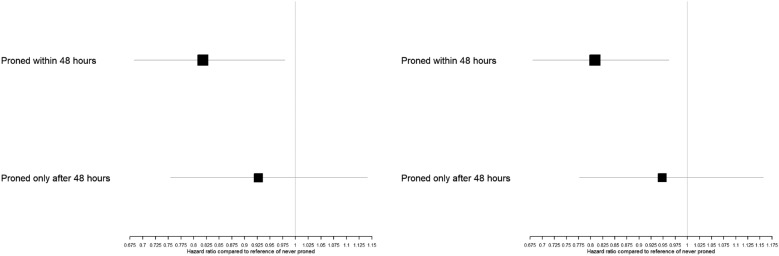
Results: 3131 patients had data on prone positioning, 1482 (47%) were never proned, 1034 (33%) were proned within 48 h and 615 (20%) were proned only after 48 h of commencement of IMV. 28-day (hazard ratio 0.82, 95% confidence interval [CI] 0.68, 0.98, p = 0.03) and 90-day (hazard ratio 0.81, 95% CI 0.68, 0.96, p = 0.02) mortality risks were lower in those patients proned within 48 h of IMV compared to those never proned. However, there was no evidence for a statistically significant association between prone positioning after 48 h with 28-day (hazard ratio 0.93, 95% CI 0.75, 1.14, p = 0.47) or 90-day mortality (hazard ratio 0.95, 95% CI 0.78, 1.16, p = 0.59).
Conclusions: Prone positioning is associated with improved outcomes in patients with COVID-19, but timing matters. We found no association between later proning and patient outcome.
Keywords: COVID-19; Cox proportional hazards models; Invasive mechanical ventilation; Prone positioning; Proning.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Participating hospitals obtained local ethics committee approval and a waiver of informed consent was granted in all cases. Consent for publication: Not applicable. Competing interests: A/Prof Li Bassi received research support from Fisher and Paykel outside the submitted work. Dr McNicholas has provided consultancy to Teleflex. Prof. Brodie receives research support from ALung Technologies, and he has been on the medical advisory boards for Baxter, Abiomed, Xenios, and Hemovent. Prof. Fraser receives research support from Fisher and Paykel, Xenios and MERA outside the submitted work. Prof. Laffey reports consulting fees from Cellenkos outside the submitted work.
Figures



References
-
- Guerin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159–68. - PubMed
