

The Inflammatory Landscape of a Whole-Tissue Explant Model of Hidradenitis Suppurativa
- PMID: 39930604
- PMCID: PMC11811487
- DOI: 10.1111/exd.70057
The Inflammatory Landscape of a Whole-Tissue Explant Model of Hidradenitis Suppurativa
Abstract
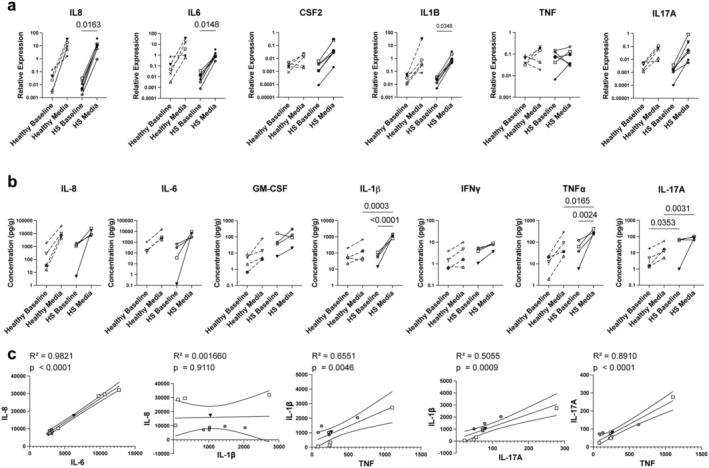
Hidradenitis suppurativa (HS) is a relatively common and highly morbid inflammatory skin disease. Due to the relatively limited understanding of HS's pathogenesis, there are currently insufficient treatment options available, and many patients' medical needs are not being met. This is partly due to the historical scarcity of ex vivo assays and animal models that accurately recapitulate the disease. Thus, we have developed a standardised whole-tissue explant model of HS to examine its pathogenic mechanisms and the efficacy of potential treatments within intact human tissue. We measured cytokine protein and RNA within whole tissue maintained in an agar-media solution, finding that IL-6 and IL-8 concentrations trended upwards in both HS explants and healthy controls, while IL-17A, IL-1β, and TNF-α exhibited increases in HS tissue alone. We also show that the explants were responsive to treatment with both dexamethasone and IL-2. Not only do our results show that this model effectively delivers treatments throughout the explants, but they also elucidate which cytokines are related to the explant process regardless of tissue state and which are related to HS tissue specifically, laying the groundwork for future implementations of this model.
Keywords: cytokine; explant model; hidradenitis suppurativa; immunology; inflammation.
© 2025 The Author(s). Experimental Dermatology published by John Wiley & Sons Ltd.
Conflict of interest statement
Michael D. Rosenblum is a consultant and cofounder of TRex Bio Inc., Sitryx Bio Inc., and Radera Bio Inc. He is also a consultant for Mozart Bio Inc. Jarish N. Cohen is a consultant for TRex Bio Inc. and Radera Bio Inc. Haley B. Naik has received consulting fees from Abbvie, Medscape, Sonoma Biotherapeutics, Union Chimique Belge's (UCB) and Novartis; and holds shares in Radera Inc. She is also an Associate Editor for JAMA Dermatology and Vice President of the Hidradenitis Suppurativa Foundation. Ryan L. Kyle and Matthew Kelly are employees of Sitryx Therapeutics.
Figures



Update of
-
A Novel Whole Tissue Explant Model of Hidradenitis Suppurativa.bioRxiv [Preprint]. 2024 Jul 23:2024.07.19.603617. doi: 10.1101/2024.07.19.603617. bioRxiv. 2024. Update in: Exp Dermatol. 2025 Feb;34(2):e70057. doi: 10.1111/exd.70057. PMID: 39211108 Free PMC article. Updated. Preprint.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
