

Immune microenvironment features underlying the superior efficacy of neoadjuvant immunochemotherapy over chemotherapy in local advanced gastric cancer
- PMID: 39931056
- PMCID: PMC11808021
- DOI: 10.3389/fimmu.2025.1497004
Immune microenvironment features underlying the superior efficacy of neoadjuvant immunochemotherapy over chemotherapy in local advanced gastric cancer
Abstract
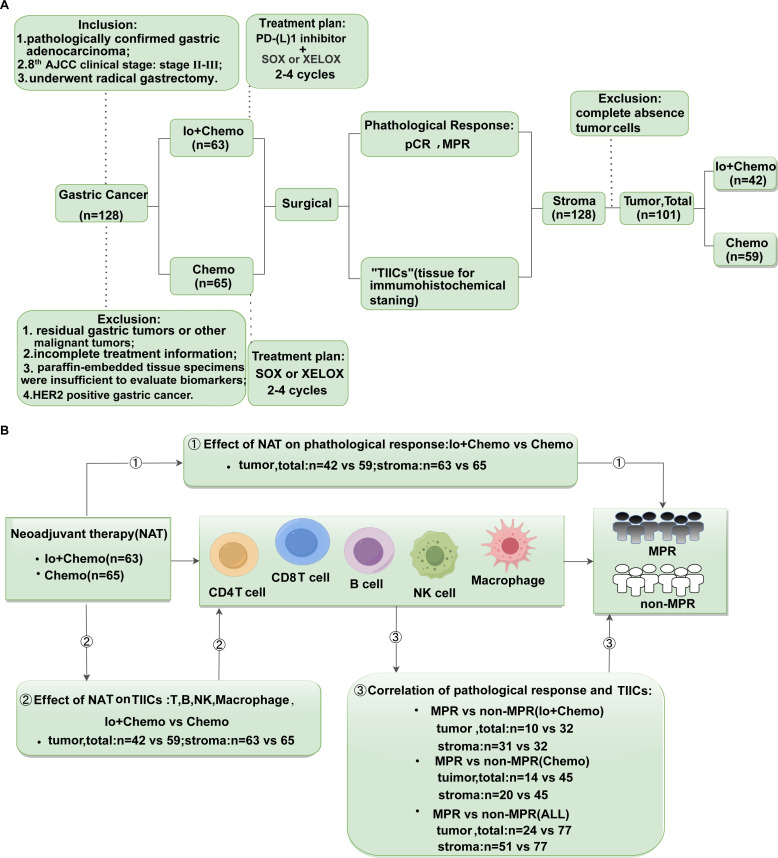
Background: The therapeutic efficacy of neoadjuvant immunotherapy combined with chemotherapy (Io+Chemo) is superior than chemotherapy alone (Chemo). However, the mechanism of Io+Chemo superiority remains to be further elucidated.
Methods: The study included 128 patients with resectable stage II-III gastric cancer, in which 63 were given neoadjuvant Io+Chemo, and 65 Chemo alone. Patients given Io+Chemo were treated with 2-4 cycles of PD-(L)1 inhibitor (Pembrolizumab, Sintililimab or Nivolumab) with S-1 and oxaliplatin (SOX) or capecitabine and oxaliplatin (XELOX) before surgical resection. Patients given Chemo were treated with 2-4 cycles of SOX or XELOX before surgical resection. Tumor tissues were evaluated for tumor-infiltrating immune cells (TIICs) using immunohistochemistry and QuPath software quantitative analysis, for detecting T, B, NK, plasma cells, and macrophages. The relationship between TIICs and different neoadjuvant treatment regimens and pathological responses was also explored.
Results: Compared with Chemo, Io+Chemo induced higher rates of pathological complete response (33.3 vs. 9.2%, p=0.001) and major pathological response (MPR) (49.2 vs. 30.8%, p=0.033). Compared with Chemo group, density of CD4+(1904.8 vs. 1530), CD8+(1982.9 vs. 1124.4), CD20+(1115.6 vs. 574), CD38+(1580.4 vs. 1128), CD138+(1237.2 vs. 496.4), and CD56+ (596.8 vs. 159) cells was increased 24.5%, 76.4%, 94.4%, 40.1%, and 149.2% respectively, whereas CD163+ macrophages (994.4 vs. 1706) was decreased 41.7% in Io+Chemo group.
Conclusions: Our study favors neoadjuvant Io+Chemo over Chemo and reveals Io+Chemo can induce the formation of an immune-activated microenvironment that make Io+Chemo superior to Chemo.
Keywords: gastric cancer; immunochemotherapy; neoadjuvant therapy; tumor immune microenvironment; tumor-infiltrating immune cells.
Copyright © 2025 Zhang, Li, Zhao, Jiang, Wang, Sun, Zhang and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Tumor microenvironment features decipher the outperformance of neoadjuvant immunochemotherapy over chemotherapy in resectable non-small cell lung cancer.Front Immunol. 2022 Oct 6;13:984666. doi: 10.3389/fimmu.2022.984666. eCollection 2022. Front Immunol. 2022. PMID: 36275670 Free PMC article.
-
TLS and immune cell profiling: immunomodulatory effects of immunochemotherapy on tumor microenvironment in resectable stage III NSCLC.Front Immunol. 2024 Dec 11;15:1499731. doi: 10.3389/fimmu.2024.1499731. eCollection 2024. Front Immunol. 2024. PMID: 39726591 Free PMC article.
-
[Safety and effectiveness of oxaliplatin combined with capecitabine or oxaliplatin combined with S-1 neoadjuvant chemotherapy in the treatment of advanced gastric cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 Feb 25;24(2):138-144. doi: 10.3760/cma.j.cn.441530-20200721-00433. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 33508919 Chinese.
-
Tumor immune microenvironment remodeling after neoadjuvant therapy in gastric cancer: Update and new challenges.Biochim Biophys Acta Rev Cancer. 2025 Jul;1880(3):189350. doi: 10.1016/j.bbcan.2025.189350. Epub 2025 May 10. Biochim Biophys Acta Rev Cancer. 2025. PMID: 40355011 Review.
-
Overview of adjuvant and neoadjuvant therapy for resectable gastric cancer in the East.Dig Surg. 2013;30(2):119-29. doi: 10.1159/000350877. Epub 2013 Jul 18. Dig Surg. 2013. PMID: 23867588 Review.
Cited by
-
Exploring NUP62's role in cancer progression, tumor immunity, and treatment response: insights from multi-omics analysis.Front Immunol. 2025 Mar 3;16:1559396. doi: 10.3389/fimmu.2025.1559396. eCollection 2025. Front Immunol. 2025. PMID: 40098960 Free PMC article.
References
-
- Schneider BJ, Shah MA, Klute K, Ocean A, Popa E, Altorki N, et al. . Phase I study of epigenetic priming with azacitidine prior to standard neoadjuvant chemotherapy for patients with resectable gastric and esophageal adenocarcinoma: evidence of tumor hypomethylation as an indicator of major histopathologic response. Clin Cancer Research: Off J Am Assoc Cancer Res. (2017) 23:2673–80. doi: 10.1158/1078-0432.CCR-16-1896 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous