

Vestibular paroxysmia: a systematic review
- PMID: 39932594
- PMCID: PMC11814022
- DOI: 10.1007/s00415-025-12913-8
Vestibular paroxysmia: a systematic review
Abstract
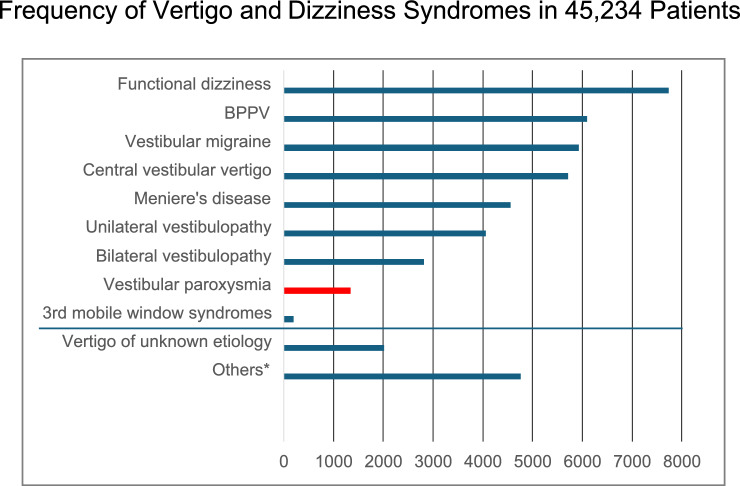
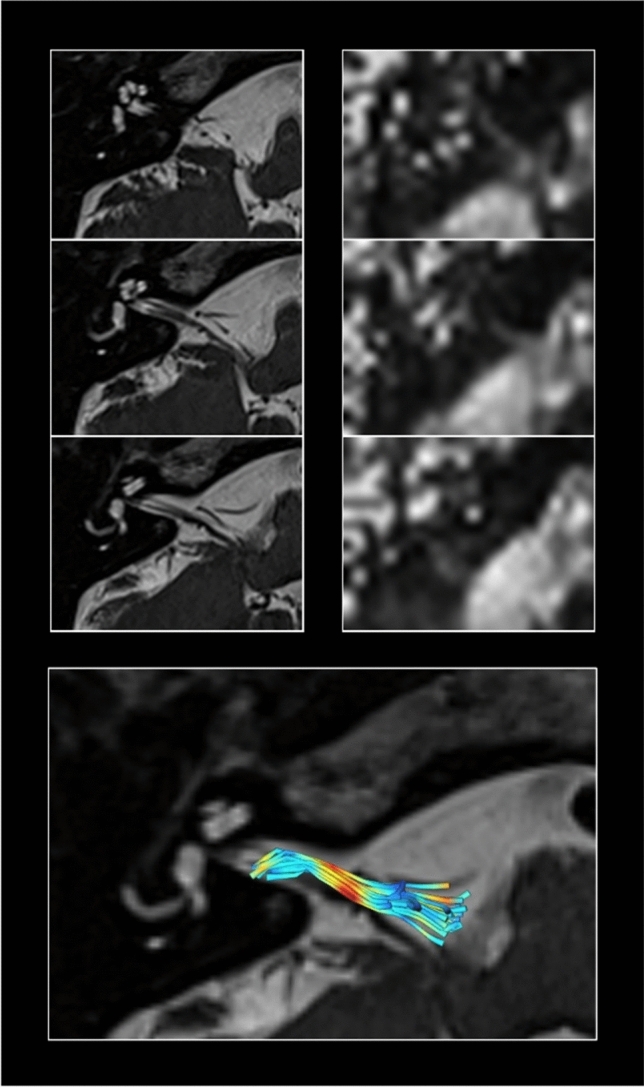
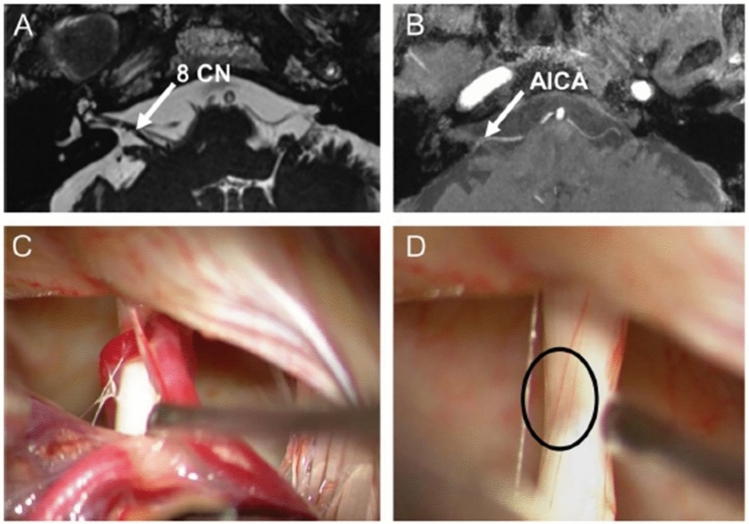
The key symptoms of vestibular paroxysmia (VP) due to neurovascular cross-compression (classical VP) or compression of the eighth nerve by space-occupying cerebellar-pontine angle processes (secondary VP) are frequent short attacks of vertigo and dizziness with unsteadiness which last seconds to minutes. They can be accompanied by unilateral auditory symptoms such as tinnitus or hyperacusis. Head movements and hyperventilation can induce nystagmus and VP attacks that most often occur spontaneously. VP is diagnosed in 3% of patients in a tertiary vertigo care center and very rarely affects children. The mean age of first appearance is 47 to 51 years with equal sex distribution. A combination of high-resolution MRI sequences (with constructive interference in steady-state/fast imaging employing steady-state, 3D-CISS/ FIESTA) of the cerebello-pontine may support the diagnosis although the beneficial treatment with sodium channel blockers is the most reliable clinical sign for classical VP, secondary VP and idiopathic VP (without verification of a causative pathology). Because of the frequency, shortness, and audiovestibular symptomatology of the attacks, the differential diagnosis to other conditions such as paroxysmal brainstem attacks, vestibular epilepsy, rotational vertebral artery compression syndrome or "near"-narrowed internal auditory canal syndrome is only relevant in exceptional cases. However, imaging of the posterior fossa including the inner ear is mandatory to distinguish between classical, secondary and idiopathic VP forms. Randomized controlled trials for medical treatment are still needed. Practical therapy of choice is medical treatment with sodium channel blockers (carbamazepine, oxcarbazepine, lacosamide). A microsurgical decompression is effective in secondary VP but is the ultimate therapy in cases with classical or idiopathic VP when medication is not tolerated.
Keywords: Audiovestibular deficits; Neurovascular cross compression; Sodium channel blockers; Vertigo attacks; Vestibular excitation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors report no conflicts of interest.
Figures

References
-
- Jannetta PJ (1975) Neurovascular cross-compression in patients with hyperactive dysfunction symptoms of the eighth cranial nerve. Surg Forum 26:467–468 - PubMed
-
- Møller MB, Møller AR, Jannetta PJ, Sekhar L (1986) Diagnosis and surgical treatment of disabling positional vertigo. J Neurosurg 64:21–28 - PubMed
-
- Møller MB, Møller AR (1990) Vascular compression syndrome of the eighth nerve. Clinical correlations and surgical findings. Neurol Clin 8(2):421–439 - PubMed
-
- Møller MB, Møller AR, Jannetta PJ, Jho HD, Sekhar LN (1993) Microvascular decompression of the eighth nerve in patients with disabling positional vertigo: selection criteria and operative results in 207 patients. Acta Neurochir 125(1–4):75–82 - PubMed
-
- Brandt T, Dieterich M (1994) Vestibular paroxysmia: vascular compression of the eighth nerve? Lancet 343(8900):798–799 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
