

Analysis of effector/memory regulatory T cells from arrhythmogenic cardiomyopathy patients identified IL-32 as a novel player in ACM pathogenesis
- PMID: 39934117
- PMCID: PMC11814135
- DOI: 10.1038/s41419-025-07364-y
Analysis of effector/memory regulatory T cells from arrhythmogenic cardiomyopathy patients identified IL-32 as a novel player in ACM pathogenesis
Abstract
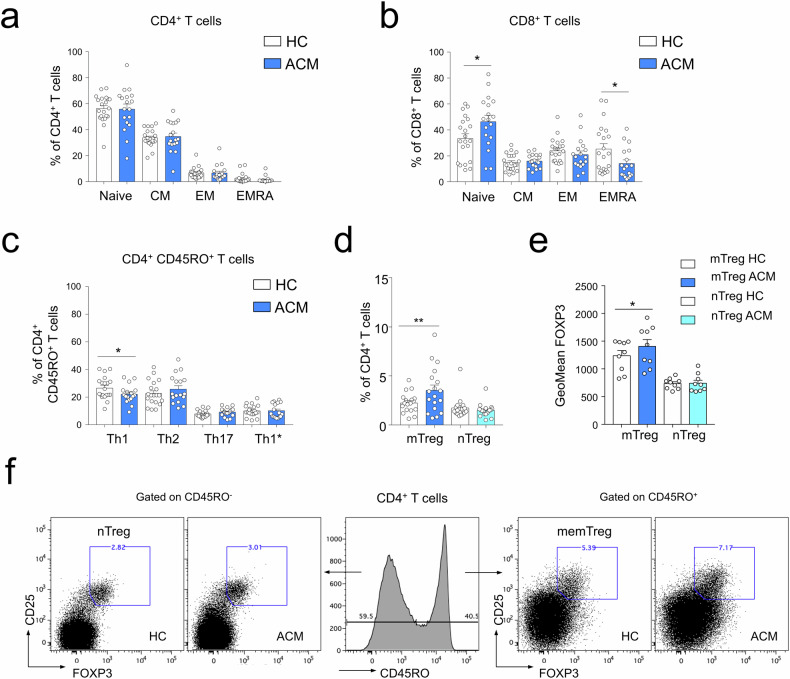
Arrhythmogenic cardiomyopathy (ACM) is an inherited cardiac disorder that causes sudden cardiac death and progressive heart failure. Besides fibro-fatty replacement and myocyte degenerative changes, inflammatory patchy infiltrates are found in myocardial histological analysis of ACM patients. Inflammatory cells could actively participate in ACM pathogenesis, contributing to the alteration of cardiac microenvironment homeostasis, thus triggering disease evolution. In order to characterize the immune-derived mediators involved in ACM pathogenesis, peripheral blood mononuclear cells from ACM patients were characterized and compared to healthy controls' ones. Flow cytometry analysis revealed a lower frequency of CD4+ T helper type 1 cells, NK cells, and terminally differentiated CD8+ EMRA+ T cells in ACM patients compared to age-matched controls. In contrast, a higher proportion of effector/memory FOXP3+ CCR4+ CD45RO+ regulatory CD4+ T cells (Treg) were found in ACM patients. Single-cell RNA-seq performed on isolated memory Treg cells (mTreg) from ACM patients and healthy controls identified 6 clusters characterized by specific gene signatures related to tissue repair and immunosuppressive pathways. Notably, interleukin 32 (IL-32) was the most differentially expressed gene in ACM patients mTreg with respect to healthy controls. Treatment of human cardiac mesenchymal stromal cells with recombinant IL-32 in vitro promoted lipid droplet accumulation and collagen deposition, thus identifying IL-32 as a new potential player in the immune-mediated trigger of cardiac fibro-fatty replacement in ACM. Overall, we here provide the first complete characterization of circulating ACM immune cells, revealing an abundance of Treg. The high expression of IL-32 in ACM Treg may contribute to accelerated cardiac remodeling in ACM patients' hearts.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
