

Minimal Invasive Pancreatoduodenectomy: A Comprehensive Systematic Review and Metanalysis of Randomized Controlled Clinical Trials
- PMID: 39937403
- PMCID: PMC11976793
- DOI: 10.1245/s10434-025-16990-x
Minimal Invasive Pancreatoduodenectomy: A Comprehensive Systematic Review and Metanalysis of Randomized Controlled Clinical Trials
Abstract
Background: The role of a minimally invasive approach (MI) in patients who underwent pancreatoduodenectomy (PD) remained unclear.
Methods: A systematic search of randomized controlled trials was conducted. A random-effects meta-analysis was conducted, reporting risk ratio (RR) or mean difference (MD). The primary endpoints were the morbidity, mortality, and R1 rate. The secondary endpoints were clinically relevant postoperative pancreatic fistula (POPF), postpancreatectomy hemorrhage (PPH), delayed gastric emptying (DGE), biliary fistula, reoperation, length of stay (LOS), time to functional recovery (TFR), and readmission.
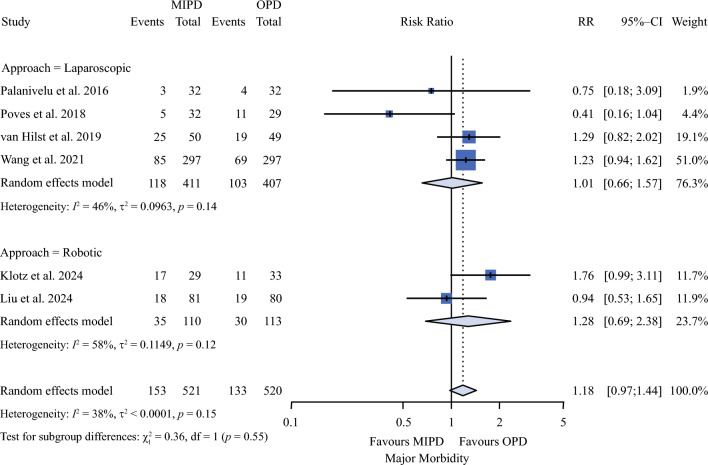
Results: The meta-analysis includes seven studies and 1428 patients: 618 (46.5%) in the OPD arm and 711 (53.5%) in minimally invasive pancreaticoduodenectomy (MIPD). The mortality rate was 2.9% for MIPD and 2.6% for OPD (RR 1.11 [range 0.53-2.29]). The major morbidity rate was 29.4% for MIPD and 25.6% for OPD (RR 1.11 [range 0.53-2.29]). The R1 rate was 6.2% for MIPD and 7% for OPD (RR 0.80 [0.54-1.20]). The operative time, comprehensive complication index score, POPF, PPH, DGE, biliary fistula, reoperation, readmission, LOS, TFR, and harvested lymph nodes were similar. Greater than 25% of heterogeneity was observed for major morbidity, operative time, POPF, LOS, TFR, and harvested lymph nodes. No publication bias was registered.
Conclusions: Minimally invasive pancreaticoduodenectomy was not superior to OPD and provided marginal advantages in short-term results. Further efforts should be addressed to clarify the impact of learning curve in MIPD results and the economic sustainability of MIPD, particularly robotic approach.
Keywords: Minimally invasive surgery; Morbidity; Mortality; Pancreatoduodenectomy.
© 2025. The Author(s).
Conflict of interest statement
Disclosure: All authors disclosed any actual or potential conflict of interest, including any financial, personal, or other relationships with other people or organizations within that could inappropriately influence (bias) this work.
Figures

References
-
- Fingerhut A, Vassiliu P, Dervenis C, Alexakis N, Leandros E. What is in a word: pancreatoduodenectomy or pancreaticoduodenectomy? Surgery. 2007;142:428–9. - PubMed
-
- Asbun HJ, Moekotte AL, Vissers FL, et al. The Miami international evidence-based guidelines on minimally invasive pancreas resection. Ann Surg. 2020;271:1–14. - PubMed
-
- Pang L, Kong J, Wang Y, Zhang Y. Laparoscopic versus open pylorus-preserving pancreatoduodenectomy. The first meta-analyse of retrospective matched cases. Acta Cir Bras. 2018;33:40–8. - PubMed
-
- Palanivelu C, Senthilnathan P, Sabnis SC, et al. Randomized clinical trial of laparoscopic versus open pancreatoduodenectomy for periampullary tumours. Br J Surg. 2017;104(11):1443–50. - PubMed
-
- Poves I, Burdío F, Morató O, et al. Comparison of perioperative outcomes between laparoscopic and open approach for pancreatoduodenectomy: The PADULAP randomized controlled trial. Ann Surg. 2018;268:731–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
