

Efficacy and safety of nivolumab plus ipilimumab in patients with metastatic variant histology (non-clear cell) renal cell carcinoma
- PMID: 39939142
- PMCID: PMC11822430
- DOI: 10.1136/jitc-2024-010958
Efficacy and safety of nivolumab plus ipilimumab in patients with metastatic variant histology (non-clear cell) renal cell carcinoma
Abstract
Background: Nivolumab plus ipilimumab (nivo/ipi) is a standard of care first-line (1 L) therapy for patients with metastatic clear-cell renal cell carcinoma (ccRCC), but its role in patients with metastatic, non-ccRCC has not been fully defined. We report a single-institution experience with nivo/ipi in non-ccRCC.
Methods: Between November 2017 and February 2024, 55 patients with metastatic non-ccRCC received nivo/ipi at MD Anderson Cancer Center. The tumor response was assessed by blinded radiologists using RECIST v1.1. The overall response rate (ORR), progression-free survival (PFS), PFS milestone, duration of response (DoR), and overall survival (OS) were determined. Next-generation sequencing (NGS) was performed on available tumor specimens.
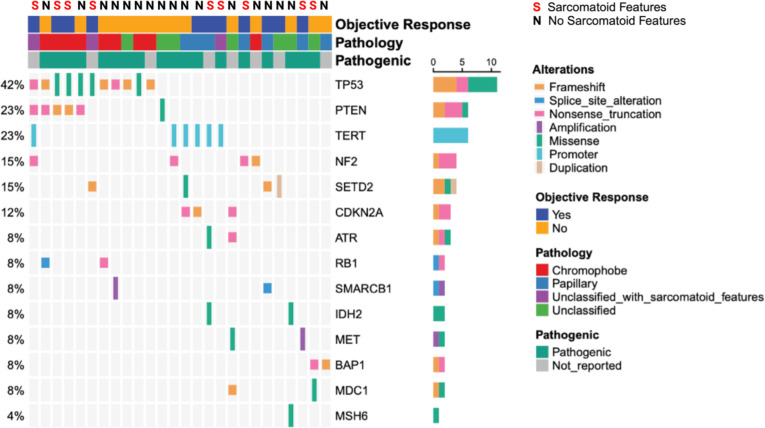
Results: Twenty-five (45.5%) patients had papillary histology (pRCC), 12 (21.8%) patients had chromophobe (chRCC), and 18 (32.7%) patients had unclassified RCC (uRCC). Fifty-two (94.5%) patients received nivo/ipi in 1 L. Sarcomatoid features (SF) were found in 20 (36.4%) cases. ORR was 48% (12/25) in pRCC, 25% (3/12) in chRCC (all 3 cases had SF), 27.8% (5/18) in uRCC, and 55% (11/20) across histologies with SF.The median PFS was 10.6 months (95% CI: 2.8 to 22.8) in pRCC, 3.6 months (95% CI: 0.9 - NE) in chRCC, and 3 months (95% CI: 2.1 to 7) in uRCC; 6-month milestone PFS was 56% (95% CI: 36.3 to 75.7), 41.7% (95% CI: 22 to 61.3), and 38.9% (95% CI: 21.7 to 56.1) in pRCC, chRCC, and uRCC, respectively. The median DoR for the entire cohort was 8.5 months (95% CI: 8 - NE). The median OS was 36.7 months (95% CI: 11.5 to 54.8) in pRCC, 25.7 months (95% CI: 0.9 - NE) in chRCC, and 11.1 months (95% CI: 6.5 - NE) in uRCC.Ten (18.2%) patients discontinued treatment due to treatment-related adverse events (AEs). Grade 3/4 immune-mediated AEs were noted in 17 (30.9%) patients. We performed NGS on 26 cases: TP53 (42%), PTEN (23%), and TERT (23%) alterations were most frequently found, with TERT and TP53 mutations enriched in pRCC and chRCC, respectively.
Conclusion: Nivo/ipi produced favorable outcomes in patients with pRCC supporting its use as 1 L therapy. Responses in patients with chRCC were noted exclusively with SF. Despite achieving an ORR of 27.8% with nivo/ipi, patients with uRCC had short PFS and inferior OS.
Keywords: Genitourinary Cancer; Immune Checkpoint Inhibitor; Immunotherapy; Kidney Cancer; Solid tumor.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: MJM, JK, NRW, KLM, TKB, YL, PR, PT, KS, HA, KME, ACJ, and SG report no disclosures. DSS reports research support from Blue Earth Therapeutics. AS reports scientific advisory board fees from Bristol Myers Squibb, Exelixis, and Pfizer; and research funding from Bristol Myers Squibb, Eisai, EMD Serono, and 4D Pharma. EH reports scientific advisory board fees from Pfizer, Eisai, and Telix Pharmaceuticals; honoraria from Targeted Oncology; and affiliations with Pelotonia Institute for Immuno-Oncology. EJ reports research funding from Arrowhead, Merck, and NiKang, as well as honoraria from Aveo, Aravive, Calithera, Eisai, Exelixis, Ipsen, Merck, NiKang, Novartis, Pfizer, and Takeda. PM reports honoraria for the service on scientific advisory boards for Mirati Therapeutics, Bristol Myers Squibb, and Exelixis; consulting for Axiom Healthcare Strategies; nonbranded educational programs supported by DAVA Oncology, Exelixis, and Pfizer; and research funding for clinical trials from Takeda, Bristol Myers Squibb, Mirati Therapeutics, Gateway for Cancer Research, and the University of Texas MD Anderson Cancer Center. MTC reports consultancy or advisory role for Astellas, AstraZeneca, AXDev, Eisai, EMD Serono, Exelixis, Genentech, Pfizer, and SeaGen; research funding from ApricityHealth, Aravive, AstraZeneca, Exelixis, Janssen, and Pfizer/EMD Serono; nonbranded educational programs from Bristol Myers Squibb, Merck, Pfizer/EMD Serono, and Roche. OA reports scientific advisory board fees from Seagen, Silverback Therapeutics, and Cardinal Health; educational program speaker from Curio Science and Aptitude Health; and research funding to the institution from AstraZeneca, Ikena Oncology, Genentech, and Arcus Biosciences. NMT reports research funding from Bristol-Myers Squibb Company (BMS), Calithera Biosciences, Nektar Therapeutics, Exelixis, Pfizer, Novartis, Arrowhead Pharmaceuticals, Mirati Therapeutics, Takeda, Epizyme, and Eisai Medical Research; consulting, advisory, travel accommodations, and expenses from BMS, Calithera Biosciences, Nektar Therapeutics, Exelixis, Pfizer, Novartis, Eisai Medical Research, Ipsen, Lilly Oncology, Neoleukin Therapeutics, Surface Oncology, ONO Pharmaceutical, and Oncorena; and honoraria from BMS, Exelixis, Nektar Therapeutics, Calithera Biosciences, Eisai Medical Research, ONO Pharmaceutical, Eli Lilly, Oncorena, Ipsen, and Surface Oncology.
Figures



References
-
- Kroeger N, Xie W, Lee J-L, et al. Metastatic non-clear cell renal cell carcinoma treated with targeted therapy agents: characterization of survival outcome and application of the International mRCC Database Consortium criteria. Cancer. 2013;119:2999–3006. doi: 10.1002/cncr.28151. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous