

Quinalizarin induces autophagy, apoptosis and mitotic catastrophe in cervical and prostate cancer cells
- PMID: 39939343
- PMCID: PMC11822151
- DOI: 10.1038/s41598-025-89847-8
Quinalizarin induces autophagy, apoptosis and mitotic catastrophe in cervical and prostate cancer cells
Abstract
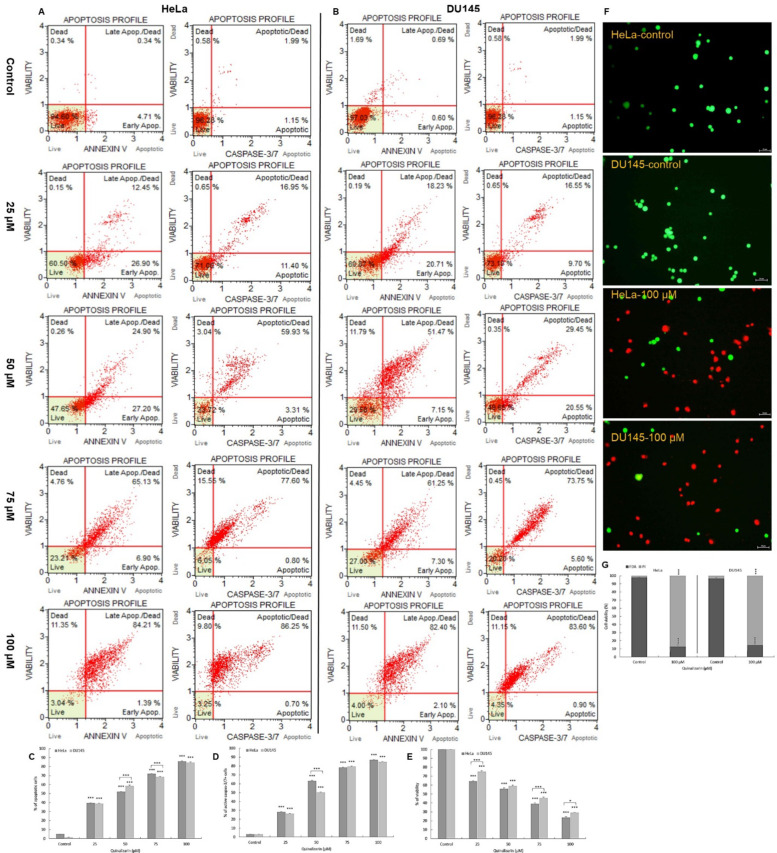
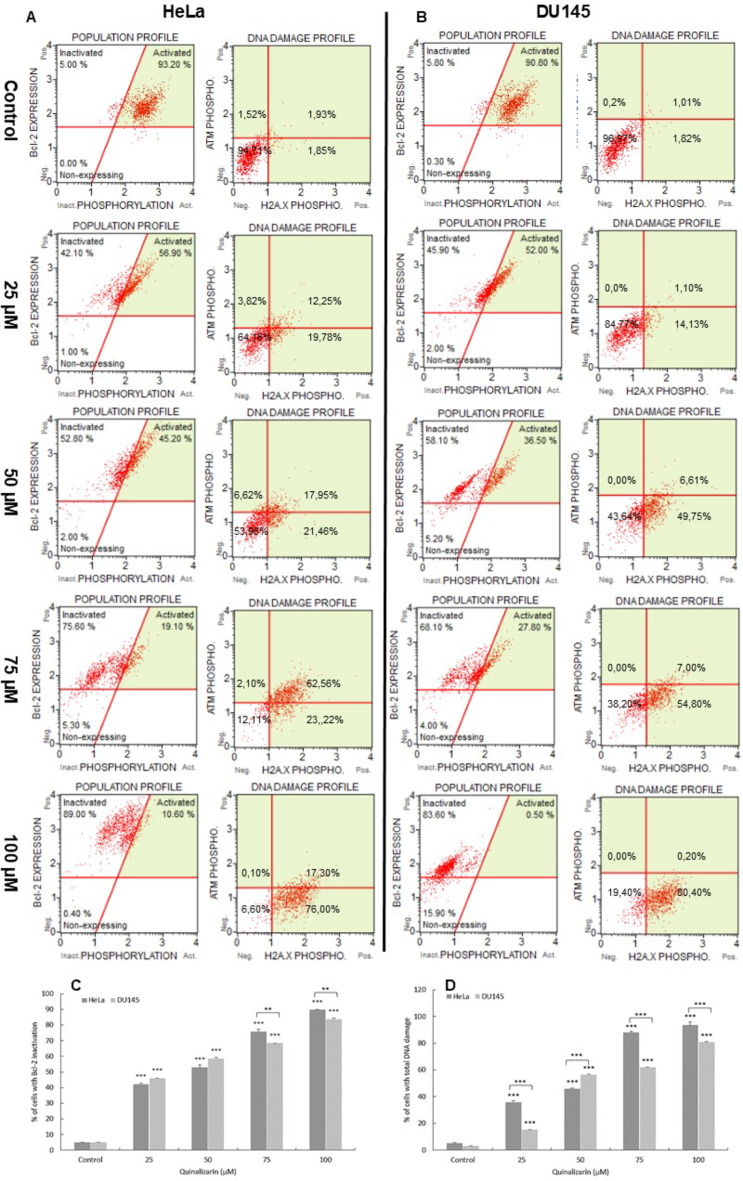
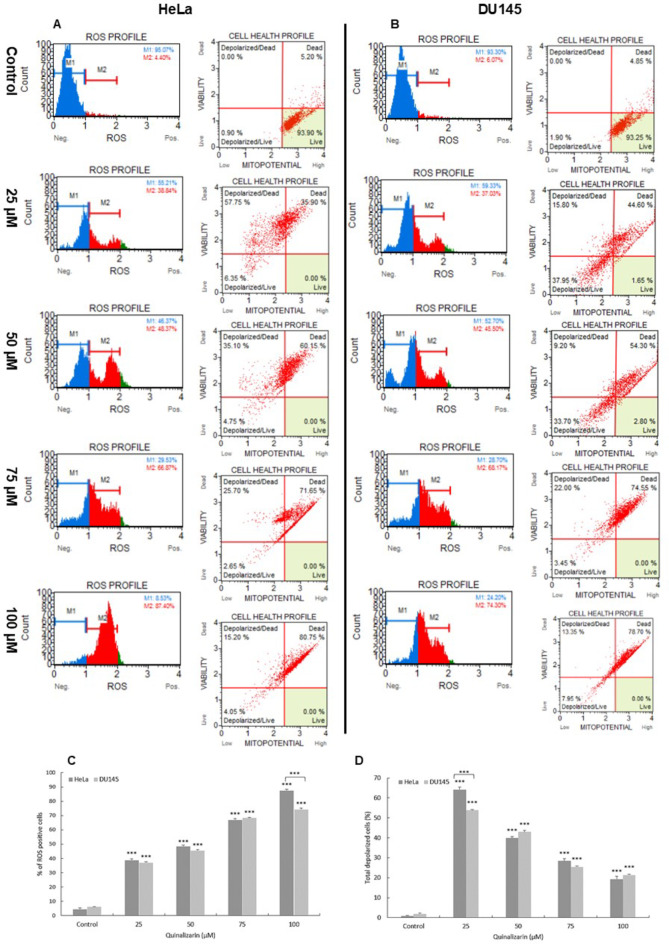
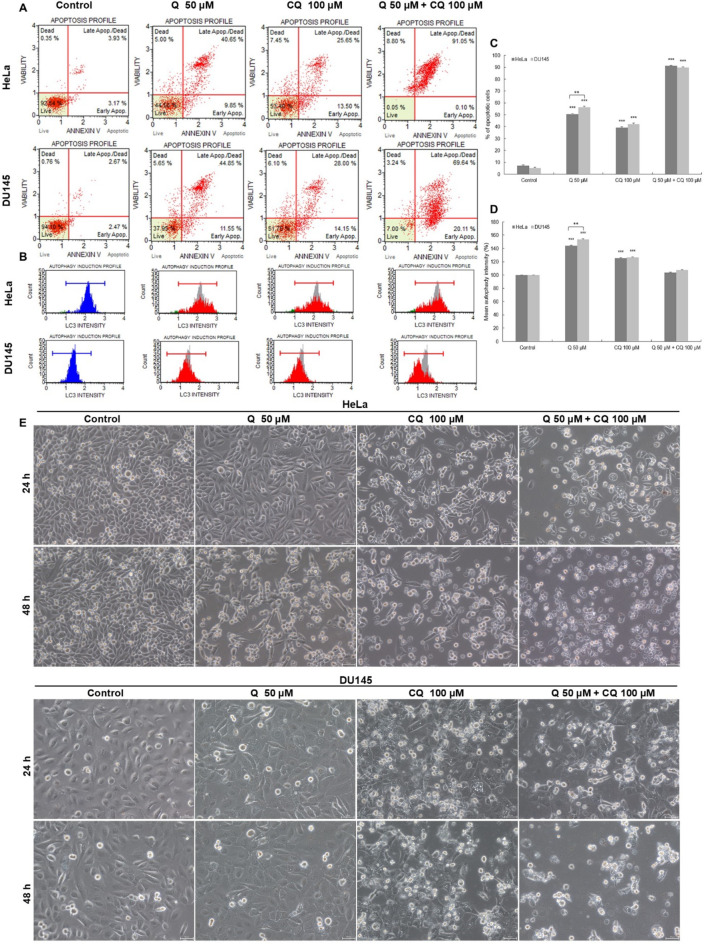
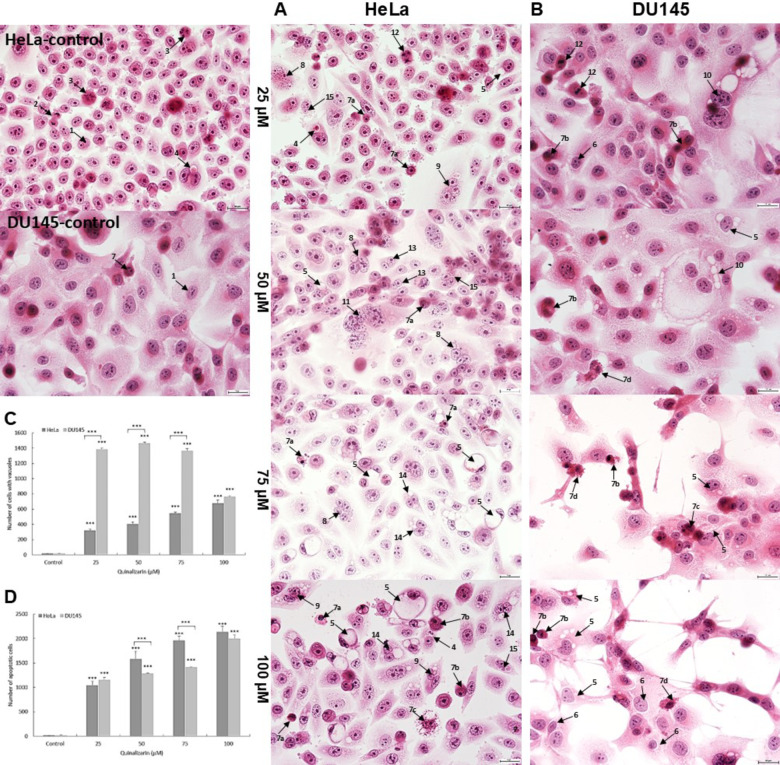
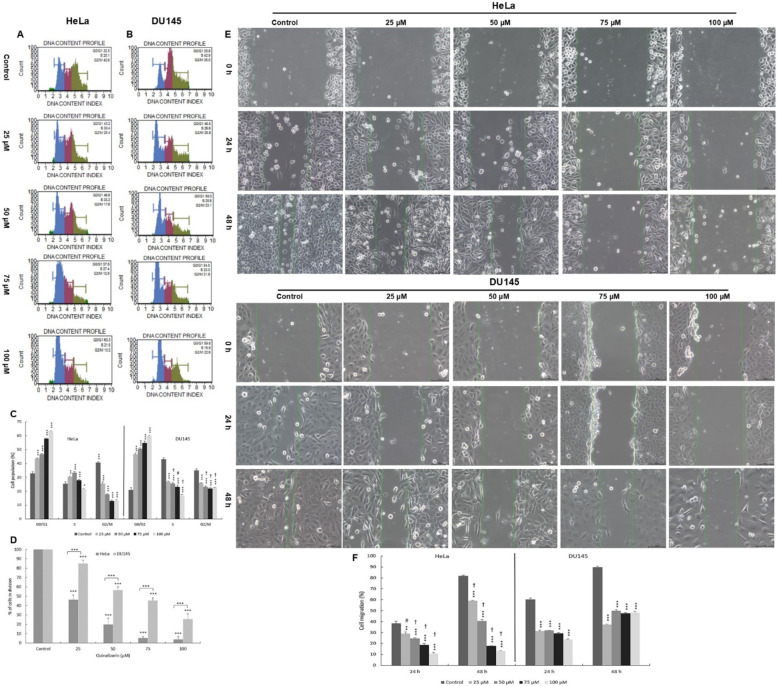
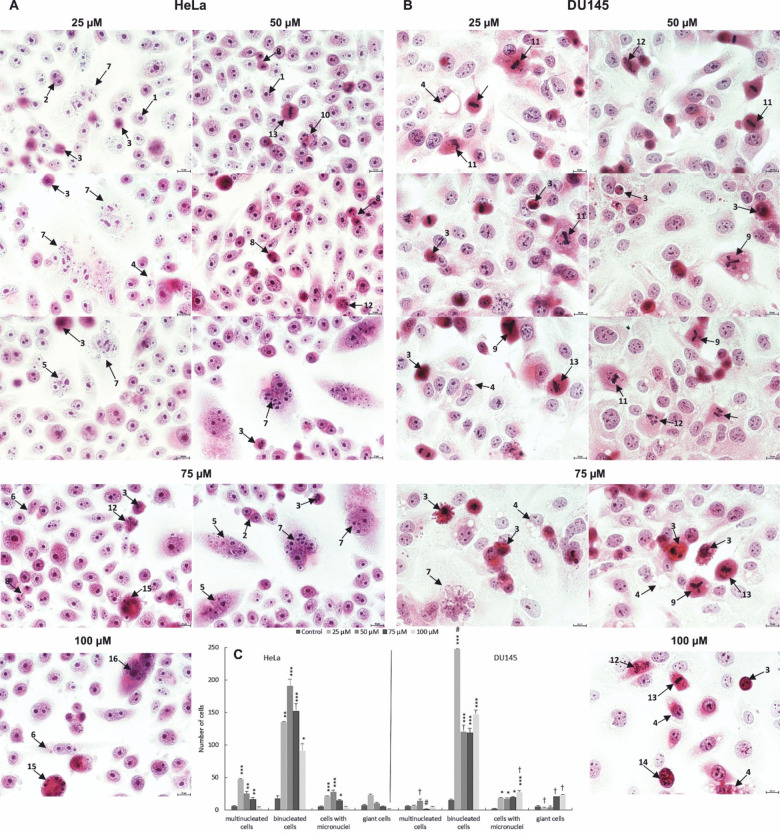
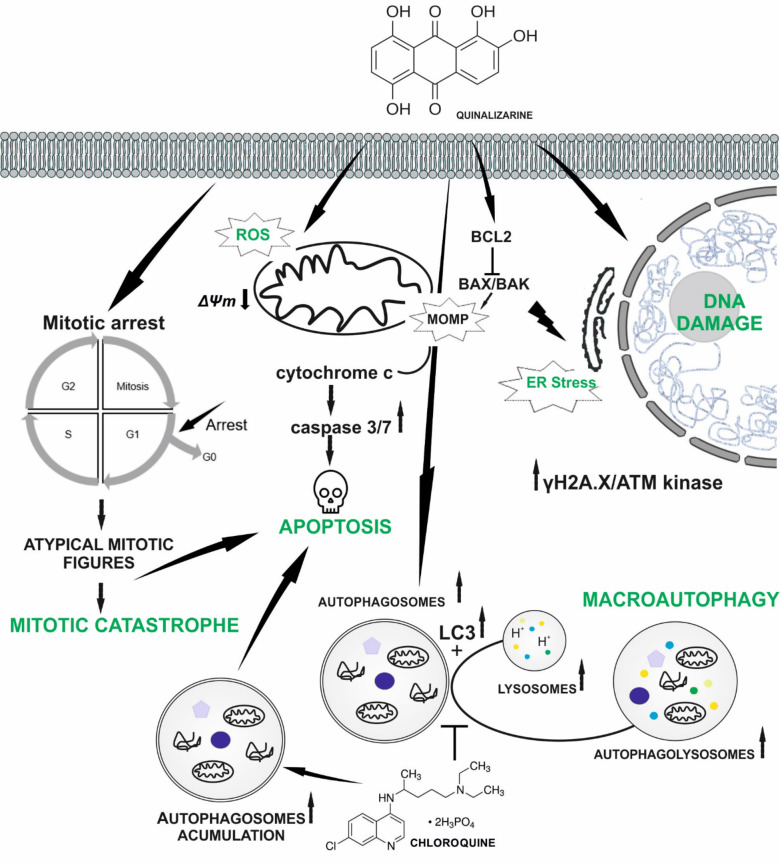
Cancer diseases are a serious health problem for society, and among them cervical and prostate cancer rank high in terms of mortality. One of the reasons is the phenomenon of drug resistance and side effects accompanying conventional chemo- and radiotherapy. This requires continuous development of alternative treatment methods and searching for new compounds with anti-cancer potential. An example is quinalizarin, which was tested for its anti-cancer potential. The MTT test showed cytotoxic activity of quinalizarin against Hela and DU145 cell lines. Morphological analysis showed nuclear changes typical of apoptosis, which was confirmed by the annexin V/PE test, activation of caspases 3/7 and inhibition of Bcl-2 protein expression. Increased permeability of mitochondrial membranes and ROS generation were demonstrated. Inhibition of cell migration, blocking in the G0/G1 phase, increased number of cells with damaged DNA and an increase in markers of mitotic catastrophe, i.e. micro- and multinucleation including the presence of abnormal mitotic figures were also observed. At the same time, increased autophagy was observed, and preincubation of cells with chloroquine inhibited this process, which contributed to the increased cytotoxicity of quinalizarin towards the tested cells. Quinalizarin has a multidirectional effect based on apoptosis and alternative types of cell death.
Keywords: Apoptosis; Autophagy; Mitotic catastrophe; Oxidative stress; Quinalizarin.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
