

Combining Colchicine and Antiplatelet Therapy to Tackle Atherothrombosis: A Paradigm in Transition?
- PMID: 39940905
- PMCID: PMC11817323
- DOI: 10.3390/ijms26031136
Combining Colchicine and Antiplatelet Therapy to Tackle Atherothrombosis: A Paradigm in Transition?
Abstract
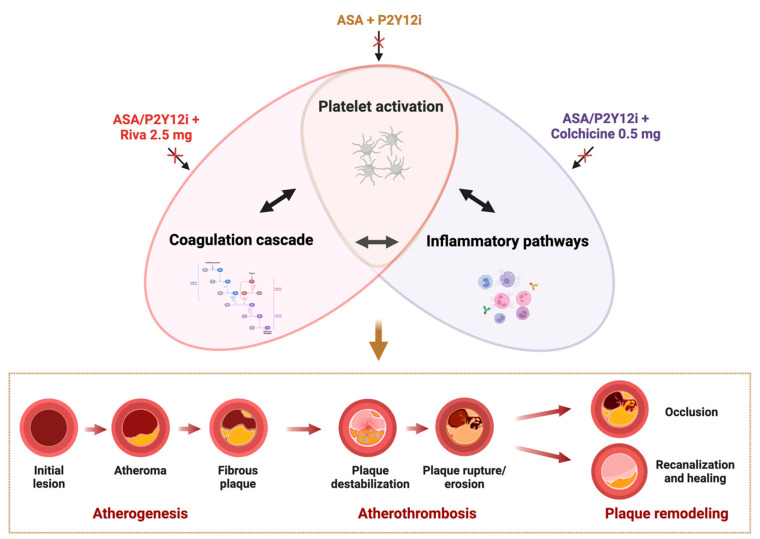
Atherothrombosis, the primary driver of acute cardiovascular (CV) events, is characterized by the activation of three key pathophysiological pathways: platelets, coagulation, and inflammation. Dual antiplatelet therapy (DAPT) is the current standard of care for patients with acute coronary syndrome, providing significant reductions in cardiovascular (CV) events, albeit with an associated increased risk of bleeding. However, the high residual risk of recurrent events among these patients highlights the need for alternative strategies to treat and prevent atherothrombosis. To this extent, several approaches aimed at targeting atherothrombosis have been proposed. Among these, a strategy of dual-pathway inhibition simultaneously targeting platelets, using single or DAPT, and coagulation, using a low-dose anticoagulant such as rivaroxaban 2.5 mg twice daily, has shown to reduce CV events but at the expense of increased bleeding. Targeting inflammatory pathways has the potential to be a highly effective strategy to tackle atherothrombosis without increasing bleeding risk. Several anti-inflammatory agents have been tested in patients with coronary artery disease, but to date only colchicine is approved for secondary prevention on top of standard care, including antiplatelet therapy. However, many aspects of colchicine's mechanism of action, including its antiplatelet effects and how it synergizes with antiplatelet therapy, remain unclear. In this review, we summarize the available clinical and pre-clinical evidence on the antiplatelet effects of colchicine and its synergistic interactions with antiplatelet therapy, highlighting their potential role in addressing atherothrombosis.
Keywords: antiplatelet; atherothrombosis; colchicine; inflammation; thrombo-inflammation.
Conflict of interest statement
D.J.A. declares that he has received consulting fees or honoraria from Abbott, Amgen, AstraZeneca, Bayer, Biosensors, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, CSL Behring, Daiichi-Sankyo, Eli Lilly, Faraday, Haemonetics, Janssen, Merck, Novartis, Novo Nordisk, PhaseBio, PLx Pharma, Pfizer, Sanofi, and Vectura, outside the present work. D.J.A. also declares that his institution has received research grants from Amgen, AstraZeneca, Bayer, Biosensors, CSL Behring, Daiichi-Sankyo, Eisai, Eli Lilly, Gilead, Janssen, Matsutani Chemical Industry Co., Merck, Novartis, Osprey Medical, Renal Guard Solutions, and Scott R. MacKenzie Foundation. The other authors have nothing to disclose.
Figures
References
-
- World Health Organization WHO Mortality Database. [(accessed on 5 November 2024)]. Available online: https://www.who.int/data/data-collection-tools/who-mortality-database.
-
- Heart Disease Facts. [(accessed on 5 November 2024)]; Available online: https://www.cdc.gov/heart-disease/data-research/facts-stats/index.html#:....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
