

Safety and Outcomes of Catheter Ablation for Consecutive Atrial Tachycardia in Elderly Patients After Previous Cardiac Interventions
- PMID: 39941346
- PMCID: PMC11818208
- DOI: 10.3390/jcm14030675
Safety and Outcomes of Catheter Ablation for Consecutive Atrial Tachycardia in Elderly Patients After Previous Cardiac Interventions
Abstract
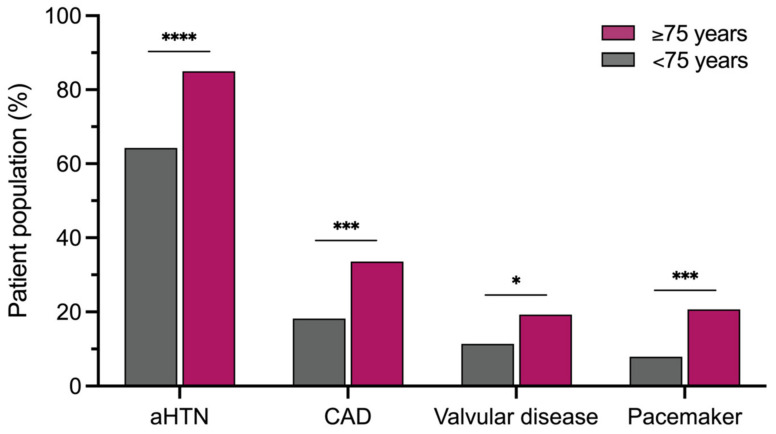
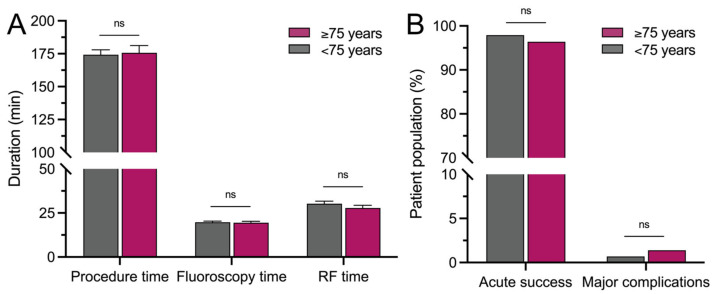
Background: Age is a relevant risk factor for the development of atrial arrhythmias and an independent predictor of adverse cardiovascular outcomes. The incidence of atrial tachycardia (AT) is known to increase with aging, but so far, there are no data on elderly patients with AT. Therefore, we sought to assess the safety and outcomes of AT ablation in patients ≥75 years compared to those <75 years. Methods: A total of 420 consecutive patients undergoing AT ablation after previous cardiac interventions (mean 2.1 ± 0.1 prior ablation procedures) were analyzed. Safety, as well as acute and mid-term outcomes of AT ablation were compared between 140 patients ≥75 years (mean age 78.1 ± 0.2 years, 22.9% aged ≥80 years (range 80-86 years)) and 280 patients <75 years (mean age 62.2 ± 0.6 years). Results: Patients ≥75 years were more often female (54.3% vs. 38.2%; p = 0.0024) and presented with more cardiac comorbidities, including arterial hypertension (85.0% vs. 64.3%; p < 0.0001) and coronary artery disease (33.6% vs. 18.2%; p = 0.0006). Acute success of AT ablation was reached in 96.4% vs. 97.9% of patients (p = 0.5173). Major complications (1.4% vs. 0.7%; p = 0.6035) and duration of hospital stay (2 (IQR 2-4) days vs. 2 (IQR 2-3) days; p = 0.9125) did not differ significantly between groups. During a follow-up of 364 (IQR 183-729.5) days, arrhythmia recurrences occurred in 45.0% vs. 49.3% (p = 0.4684), whereas repeat ablation was less frequently performed in patients ≥75 years (25.7% vs. 36.1%; p = 0.0361). Conclusions: AT ablation in patients ≥75 years after previous cardiac interventions in tertiary arrhythmia centers is safe and effective. Therefore, AT ablation should not be ruled out in elderly patients due to age alone, but should be considered based on arrhythmia burden, symptom severity and concomitant clinical and procedural risk factors.
Keywords: atrial fibrillation; atrial tachycardia; catheter ablation; elderly patients; electroanatomical mapping.
Conflict of interest statement
A.-K.K. is an invited fellow of the Boston Scientific German Heart Rhythm Fellowship and has received an educational grant from Johnson & Johnson and travel grants from Abbott. F.-A.A. is an alumni fellow of the Boston Scientific German Heart Rhythm Fellowship, a speaker for Bristol Myers Squibb, and has received travel grants from Bayer Pharmaceuticals. C.M. has received fees as a speaker and for participating in advisory boards from Abbott, Bayer, Biotronik, Biosense Webster, BMS, Boston Scientific, Daiichi Sankyo, Philips Research Europe, and Pfizer. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

Similar articles
-
Advanced electrophysiologic mapping systems: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(8):1-101. Epub 2006 Mar 1. Ont Health Technol Assess Ser. 2006. PMID: 23074499 Free PMC article.
-
Effect of Catheter Ablation Using Pulmonary Vein Isolation With vs Without Posterior Left Atrial Wall Isolation on Atrial Arrhythmia Recurrence in Patients With Persistent Atrial Fibrillation: The CAPLA Randomized Clinical Trial.JAMA. 2023 Jan 10;329(2):127-135. doi: 10.1001/jama.2022.23722. JAMA. 2023. PMID: 36625809 Free PMC article. Clinical Trial.
-
Atrial tachycardia ablation in patients with a functional single ventricle after the Fontan surgery.Kardiol Pol. 2016;74(8):762-771. doi: 10.5603/KP.a2015.0214. Epub 2015 Nov 17. Kardiol Pol. 2016. PMID: 26575308
-
Cardiovascular outcomes of patients with atrial fibrillation and concomitant cardiac amyloidosis undergoing percutaneous catheter ablation.Curr Probl Cardiol. 2025 Mar;50(3):102953. doi: 10.1016/j.cpcardiol.2024.102953. Epub 2024 Dec 2. Curr Probl Cardiol. 2025. PMID: 39631636 Review.
-
Long-term outcomes of catheter ablation for atrial fibrillation in octogenarians.J Interv Card Electrophysiol. 2024 Aug 14. doi: 10.1007/s10840-024-01879-8. Online ahead of print. J Interv Card Electrophysiol. 2024. PMID: 39141267 Review.
References
-
- Eckardt L., Sehner S., Suling A., Borof K., Breithardt G., Crijns H., Goette A., Wegscheider K., Zapf A., Camm J., et al. Attaining sinus rhythm mediates improved outcome with early rhythm control therapy of atrial fibrillation: The EAST-AFNET 4 trial. Eur. Heart J. 2022;43:4127–4144. doi: 10.1093/eurheartj/ehac471. - DOI - PMC - PubMed
-
- Hijazi Z., Lindbäck J., Alexander J.H., Hanna M., Held C., Hylek E.M., Lopes R.D., Oldgren J., Siegbahn A., Stewart R.A.H., et al. The ABC (age, biomarkers, clinical history) stroke risk score: A biomarker-based risk score for predicting stroke in atrial fibrillation. Eur. Heart J. 2016;37:1582–1590. doi: 10.1093/eurheartj/ehw054. - DOI - PMC - PubMed
-
- Krijthe B.P., Kunst A., Benjamin E.J., Lip G.Y.H., Franco O.H., Hofman A., Witteman J.C.M., Stricker B.H., Heeringa J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur. Heart J. 2013;34:2746–2751. doi: 10.1093/eurheartj/eht280. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
