

Disease Progression in Charcot-Marie-Tooth Disease Type 4B (CMT4B) Associated With Mutations in Myotubularin-Related Proteins 2 and 13
- PMID: 39943887
- PMCID: PMC11822262
- DOI: 10.1111/ene.70084
Disease Progression in Charcot-Marie-Tooth Disease Type 4B (CMT4B) Associated With Mutations in Myotubularin-Related Proteins 2 and 13
Abstract
Background and aims: In 2019, we conducted a cross-sectional study, collecting information on 50 patients with CMT4B, an ultrarare CMT subtype, to better define the clinical phenotype. We now aimed at investigating disease progression in 26 patients with CMT4B1/CMT4B2, recruited from the previous study and among the Inherited Neuropathy Consortium.
Materials and methods: We retrospectively analysed disease progression in patients with CMT4B1/CMT4B2, collecting MRC scores from nine muscle pairs, Charcot-Marie-Tooth Examination Score (CMTES), and a minimal dataset of clinical information (walking difficulties, aids dependency, upper limb impairment, cranial nerves involvement) at baseline and follow-up visits. Thirteen centres from four continents were involved.
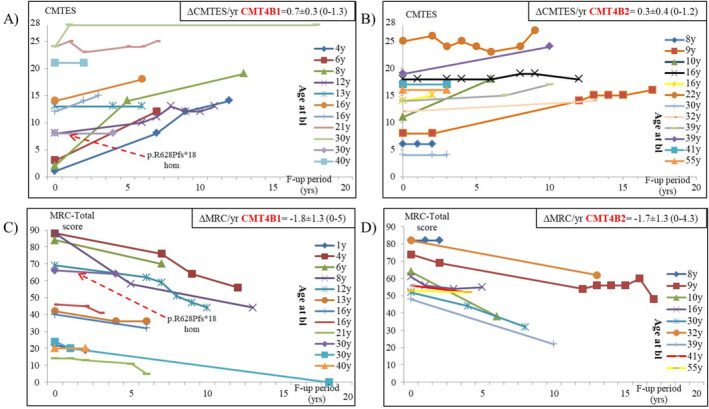
Results: Thirteen CMT4B1 and 13 CMT4B2 patients were followed up for 7.1 ± 4.9 and 7.9 ± 4.5 years, respectively. During follow-up, walking aid dependency increased: two CMT4B1 patients adopted AFOs (overall 11/12 at follow-up), and one started using wheelchair (6/12 at follow-up) at the age of 19; among CMT4B2 patients, two more required unilateral support in walking (4/11 at follow-up) by the age of 33 and 49 years, respectively. We found that disease progression, as measured by CMTES, was faster in CMT4B1 as compared to CMT4B2 patients (ΔCMTES/year 0.7 vs. 0.3, p = 0.037) but tended to slow down over time as burden of disease increased. At the end of follow-up, CMT4B1 was associated to higher disability.
Conclusions: This international collective effort enabled collection of relevant data for characterizing natural history and estimating disease progression of CMT4B1/CMT4B2 ultrarare diseases, aiming at improving their management and paving the way for designing future clinical trials.
Keywords: CMT4B; Charcot‐Marie‐Tooth disease; neuromuscular.
© 2025 The Author(s). European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
M.L. received financial grants (honoraria and speaking) from Ackea, Alnylam, AstraZeneca, Sobi, and Pfizer, and travel grants from Ackea, Alnylam, Sobi, Pfizer, Kedrion, and Grifols. S.S.S. actively serves as a consultant to Applied Therapeutics, Novartis, and Toray Industries and has research support from the National Institutes of Health, Muscular Dystrophy Association, and the Charcot‐Marie‐Tooth Association, and Applied Therapeutics. D.P. acknowledges payments or reimbursement for consultancy and participation in Advisory Boards of Inflectis, Alnylam, Akcea, Arvinas, Augustine Tx, DTx, speaker honorarium from Alnylam, participation as local PI in clinical trials sponsored by Alnylam, Ionis, AT Therapeutics, Nido‐Biosciences. S.S. acknowledges payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Lupin, Fulcrum therapeutics, payment for expert testimony from Alexys, Ology, support for attending meetings and/or travel from Biogen, Sanofi, UCB, and Fulcrum therapeutics. A. Bertini., M.M.R., C.P., S.C.P., Y.P., E.B., M.L., J.B., S.A., T.S., M.B., S.N., M.T., A.G., P.V., R.A.L., R.H., A.A.Z., M.S., S.T., F.M., D.N.H., N.K., K.W., A. Bolino., and M.E.S. have no conflicts of interest.
Figures
References
-
- Pareyson D. and Marchesi C., “Diagnosis, Natural History, and Management of Charcot‐Marie‐Tooth Disease,” Lancet Neurology 8 (2009): 654–667. - PubMed
-
- Previtali S. C., Quattrini A., and Bolino A., “Charcot‐Marie‐Tooth Type 4B Demyelinating Neuropathy: Deciphering the Role of MTMR Phosphatases,” Expert Reviews in Molecular Medicine 9 (2007): 1–16. - PubMed
-
- Bolino A., Muglia M., Conforti F. L., et al., “Charcot‐Marie‐Tooth Type 4B Is Caused by Mutations in the Gene Encoding Myotubularin‐Related Protein‐2,” Nature Genetics 25 (2000): 17–19. - PubMed
-
- Azzedine H., Bolino A., Taieb T., et al., “Mutations in MTMR13, a New Pseudophosphatase Homologue of MTMR2 and Sbf1, in Two Families With an Autosomal Recessive Demyelinating Form of Charcot‐Marie‐Tooth Disease Associated With Early‐Onset Glaucoma,” American Journal of Human Genetics 72 (2003): 1141–1153. - PMC - PubMed
-
- Senderek J., Bergmann C., Weber S., et al., “Mutation of the SBF2 Gene, Encoding a Novel Member of the Myotubularin Family, in Charcot‐Marie‐Tooth Neuropathy Type 4B2/11p15,” Human Molecular Genetics 12 (2003): 349–356. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
