

Association of baseline inflammatory biomarkers and clinical outcomes in patients with advanced renal cell carcinoma treated with immune checkpoint inhibitors
- PMID: 39943944
- PMCID: PMC11815817
- DOI: 10.1177/17588359251316243
Association of baseline inflammatory biomarkers and clinical outcomes in patients with advanced renal cell carcinoma treated with immune checkpoint inhibitors
Abstract
Background: Immune checkpoint inhibitors (ICIs) have become the mainstay treatment of metastatic kidney cancer, demonstrating enhanced outcomes and durable responses in select patient subgroups. However, identifying reliable prognostic biomarkers for treatment outcomes remains challenging.
Objectives: This study aimed to assess the correlation between baseline inflammatory markers and overall survival (OS), progression-free survival (PFS), and clinical benefit (CB) in metastatic kidney cancer patients receiving ICIs. CB was defined as patients achieving stable disease, partial response, or complete response.
Design: Retrospective, single-center study.
Methods: A retrospective analysis was conducted on 401 adult patients with advanced kidney cancer treated with ICIs at Emory Winship Cancer Institute between 2018 and 2023. Modified Glasgow Prognostic Score (mGPS), neutrophil-to-lymphocyte (NLR), monocyte-to-lymphocyte (MLR), platelet-to-lymphocyte (PLR), and neutrophil-to-eosinophil ratios (NER) were collected from baseline blood samples.
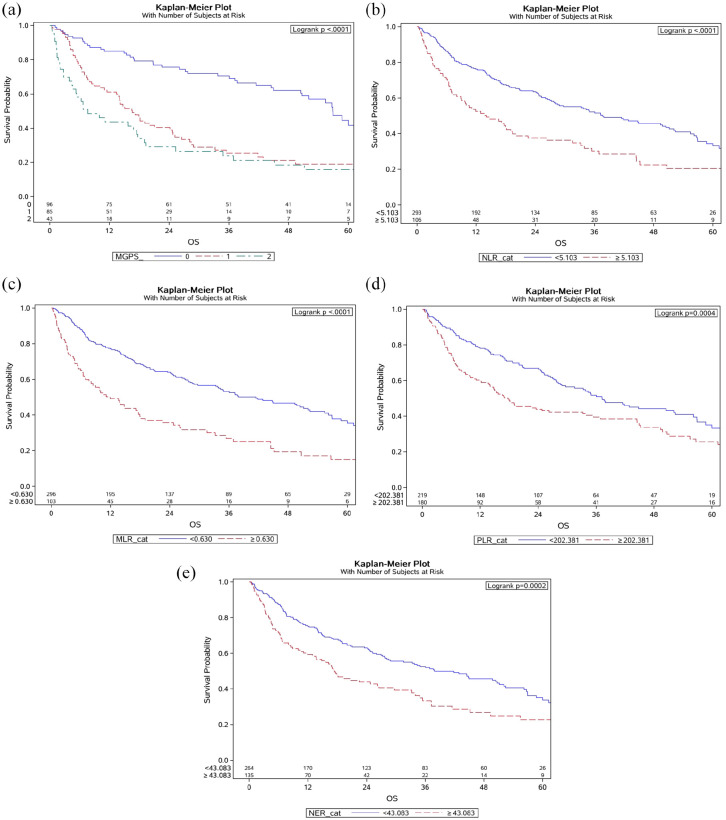
Results: Among 401 patients (median age, 66; 71% male; 21% Black/African American), median follow-up was 43.0 months (95% CI, 36.6-51.4). Patients with mGPS scores of 0 had longer OS than those with a score of 1 (hazard ratio (HR), 0.38; 95% CI, 0.23-0.62; p < 0.001) and 2 (HR, 0.37; 95% CI, 0.20-0.67; p = 0.001), and longer PFS compared to patients with mGPS scores of 1 (HR, 0.66; 95% CI, 0.44-0.98; p = 0.039) and 2 (HR, 0.44; 95% CI, 0.29-0.67; p < 0.001). Low baseline NLR was associated with longer PFS (HR, 0.73; 95% CI, 0.54-0.97; p = 0.032). Low baseline MLR correlated with improved OS (HR, 0.60; 95% CI, 0.44-0.83; p = 0.002) and PFS (HR, 0.73; 95% CI, 0.55-0.97; p = 0.031). Similarly, low baseline PLR was associated with higher CB likelihood (odds ratio (OR), 2.20; 95% CI, 1.31-3.69; p = 0.003), and low baseline NER was linked to improved OS (HR, 0.63; 95% CI, 0.46-0.87; p = 0.004), PFS (HR, 0.67; 95% CI, 0.51-0.88; p = 0.003), and higher CB (OR, 2.04; 95% CI, 1.20-3.46; p = 0.008).
Conclusion: Lower levels of systemic inflammatory markers are associated with more favorable clinical outcomes with ICI treatment. Prospective studies are needed for further validation.
Keywords: biomarkers; checkpoint inhibitors; immunotherapy; inflammation; inflammatory biomarkers; renal cell carcinoma.
© The Author(s), 2025.
Conflict of interest statement
B.N. acted as a consultant or member of the advisory board for Exelixis, IntrinsiQ Specialty Solutions, Cardinal Health, Intellisphere, and Neogenomics, received an honorarium from Catamount Medical Education, and received grants to Emory University from Xencor, Merck, Astellas, and /Pfizer for work done outside the current study. J.T.B. reports grants/contracts from Medicenna, Merck Sharp & Dohme, Surface Oncology, and Xencor; personal/consulting fees from Exelixis Inc. and Gilead Sciences Inc.; and support for other professional activities from Xencor outside the submitted work. B.C.C. reports personal/consulting fees from Bristol Myers Squibb and Gilead Research Foundation outside the submitted work. V.A.M. reports support for professional activities from Ethicon outside the submitted work. M.A.B. reports personal/consulting fees from and/or service on an advisory board of AstraZeneca, Bayer, Bristol Myers Squibb, Calithera Biosciences, Eisai Inc., EMD Serono, Exelixis Inc., Genomic Health, Janssen, Nektar, Pfizer, SeaGen, and Sanofi; and grants to his institution from AAA, AstraZeneca, Bayer, Bristol Myers Squibb, Genentech/Roche, Genome & Company, Incyte, Merck, Nektar, Peloton Therapeutics, Pfizer, SeaGen, Tricon Pharmaceuticals, and Xencor outside the submitted work. The remaining authors disclosed no conflicts of interest.
Figures

References
-
- Siegel RL, Miller KD, Wagle NS, et al.. Cancer statistics, 2023. CA Cancer J Clin 2023; 73: 17–48. - PubMed
-
- SEER*Explorer. SEER Cancer Statistics, an interactive website for SEER cancer statistics, https://seer.cancer.gov/statistics-network/explorer/ (2023, accessed 23 October 2023).
-
- Saliby RM, Saad E, Kashima S, et al.. Update on biomarkers in renal cell carcinoma. Am Soc Clin Oncol Educ Book 2024; 44: e430734. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
