

Disparity in endoscopic localisation of early distal colorectal cancers: a retrospective cohort analysis from a single institution
- PMID: 39945868
- PMCID: PMC11825640
- DOI: 10.1007/s00423-025-03642-7
Disparity in endoscopic localisation of early distal colorectal cancers: a retrospective cohort analysis from a single institution
Abstract
Background: Accurate staging of distal colorectal cancers is paramount in guiding neoadjuvant therapy, peri-operative, and ostomy planning. Early colonic lesions can be difficult to visualise on computed tomography (CT) scans, with tumour location solely deduced via endoscopy with the potential for introducing error. We aimed to address the paucity in literature in this area and assessed the accuracy of radiological and endoscopic localisation of distal colorectal cancers.
Methods: Retrospective analysis of an electronic database of patients at a large District General Hospital (DGH) diagnosed with distal colorectal cancer between January 2014 to January 2023 was performed. Patient demographics, investigations, endoscopic, and operative findings were analysed. Outcomes were assessed to determine disparities between pre-operative endoscopy and final tumour location.
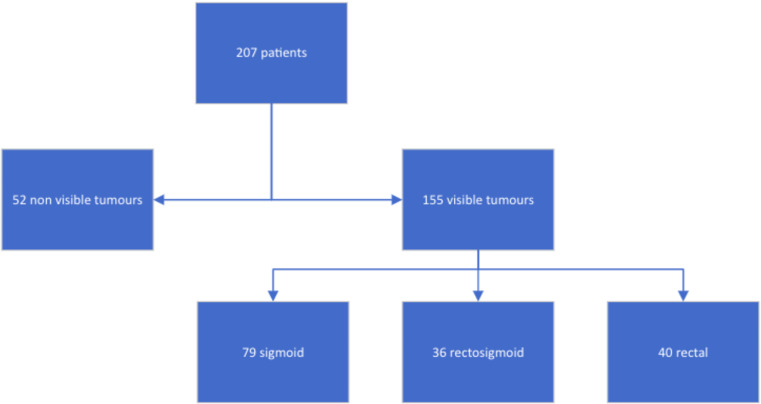
Results: A total of 212 patients were endoscopically diagnosed with distal sigmoid tumour. Of these, 207 (97.6%) had a CT scan performed with 25.1% (52/207) lesions not being identified on this imaging modality with the remainder (74.9%; 155/207) being reported as visible. 38.2% (79/207) of tumours were in the sigmoid colon, 17.4% (36/207) rectosigmoid, and 19.3% (40/207) in the rectum. Pre-operative magnetic resonance imaging (MRI) was performed in 42.5% (90/212) of cases showing 84 tumours: 6.0% (5/84) sigmoid colon, 9.5% (8/84) rectosigmoid and 83.3% (70/84) rectal cancers (upper: 34, mid-rectum: 26, low: 10), with one anal cancer. 42.3% (22/52) of patients with non-visible lesions on CT had MRI scans: 68.2% (15/22) had rectal cancer (upper: 10, mid-rectum: 4, low: 1). Of the 30 where MRI was not performed, 46.7% (14) had sigmoid cancer, 16.7% (5) rectosigmoid, and 33.3% (10) rectal intraoperatively. Overall, 30.7% (65/212) of patients reported as having a distal sigmoid lesion endoscopically in fact had rectal cancer intra-operatively (rectosigmoid lesions excluded).
Conclusion: Endoscopic localisation of distal colorectal tumours can be unreliable for accurate staging and operative planning. A pre-operative MRI scan should be considered in such instances, and particularly for non-visible lesions on CT scan. This may improve peri-operative planning, staging accuracy and patient outcomes.
Keywords: Endoscopy; MRI; Rectal cancer; Sigmoid cancer.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Approval from the local research committee was gained, and ethical approval was waived as the current study did not influence or alter the management course or treatment of any patients analysed. Competing interests: The authors declare no competing interests.
Figures


References
-
- Piscatelli N, Hyman N, Osler T (2005) Localizing colorectal cancer by colonoscopy. Arch Surg Chic Ill 1960 140(10):932–935 - PubMed
-
- Offermans T, Vogelaar FJ, Aquarius M, Janssen-Heijnen MLG, Simons PCG (2017) Preoperative segmental localization of colorectal carcinoma: CT colonography vs. optical colonoscopy. Eur J Surg Oncol 43(11):2105–2111 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
