

"Trapdoor" Medial Scapula Osteotomy for Resection of a Benign Subscapular Neoplasm: A Case Report
- PMID: 39946504
- PMCID: PMC11822220
- DOI: 10.2106/JBJS.CC.24.00338
"Trapdoor" Medial Scapula Osteotomy for Resection of a Benign Subscapular Neoplasm: A Case Report
Abstract
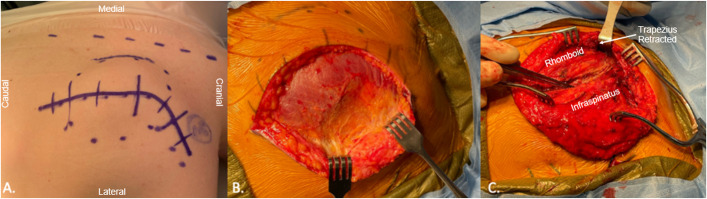
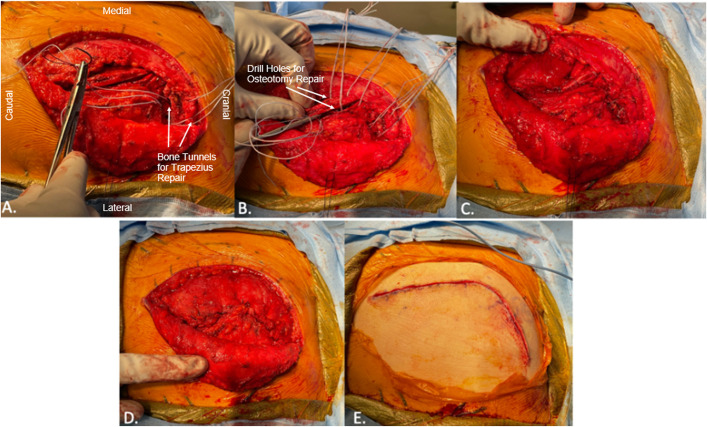
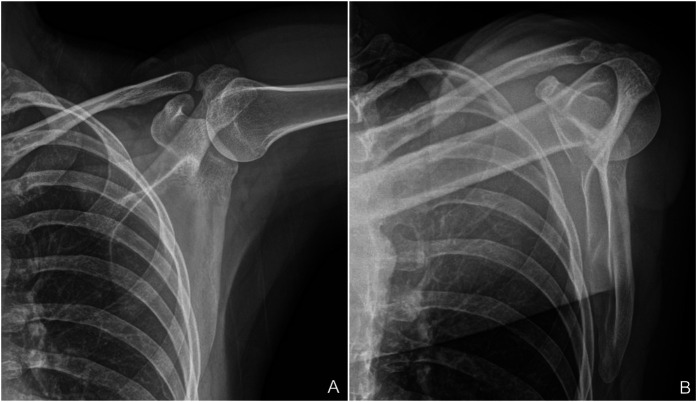
Case: Neurofibromatosis type 2 (NF2) is an autosomal dominant condition characterized by the development of neoplasms, which infrequently arise in the subscapular fossa. Surgical removal of large subscapular tumors carries the risk of shoulder dysfunction due to muscle or nerve injury. We describe the case of a patient with NF2 who presented with a hybrid subscapular neurofibroma and schwannoma tumor that was completely resected through a muscle-sparing medial scapular osteotomy approach.
Conclusion: We describe a unique muscle-sparing scapula splitting surgical approach to the subscapular region that provides excellent exposure for tumor removal and clinical outcomes with minimal postoperative scapular dyskinesis.
Level of evidence: IV (case report).
Copyright © 2025 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated.
Conflict of interest statement
Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSCC/C549).
Figures






Similar articles
-
Peripheral nerve sheath tumors in Neurofibromatosis Type 2: Surgical and histopathologic features.Clin Neurol Neurosurg. 2020 Mar;190:105649. doi: 10.1016/j.clineuro.2019.105649. Epub 2019 Dec 23. Clin Neurol Neurosurg. 2020. PMID: 31881415
-
Go for the Gold: A "Plane" and Simple Technique for Resecting Benign Peripheral Nerve Sheath Tumors.Oper Neurosurg. 2020 Jan 1;18(1):60-68. doi: 10.1093/ons/opz034. Oper Neurosurg. 2020. PMID: 30888029
-
[Judet posterior approach to the scapula].Acta Chir Orthop Traumatol Cech. 2008 Dec;75(6):429-35. Acta Chir Orthop Traumatol Cech. 2008. PMID: 19149999 Czech.
-
Giant intraosseous schwannoma of scapula: a rare case report and review of the literature.Diagn Pathol. 2014 Feb 7;9:31. doi: 10.1186/1746-1596-9-31. Diagn Pathol. 2014. PMID: 24507572 Free PMC article. Review.
-
Schwannoma and neurofibroma of the posterior tibial nerve presenting as tarsal tunnel syndrome: review of the literature with two case reports.Foot (Edinb). 2017 Aug;32:22-26. doi: 10.1016/j.foot.2017.03.005. Epub 2017 Mar 30. Foot (Edinb). 2017. PMID: 28624667 Review.
References
-
- Evans DG, Huson SM, Donnai D, Neary W, Blair V, Newton V, Harris R. A clinical study of type 2 neurofibromatosis. Q J Med. 1992;84(304):603-18. - PubMed
-
- Goel DP, Drosdowech DS, Turner RG, Lawendy AR, Garvin G. Periarticular neurofibroma of the shoulder: a case report. J Bone Joint Surg Am. 2010;92(3):715-20. - PubMed
-
- Lee DH, Hills JM, Jordanov MI, Jaffe KA. Common tumors and tumor-like lesions of the shoulder. J Am Acad Orthop Surg. 2019;27(7):236-45. - PubMed
-
- Ferner RE, O'Doherty MJ. Neurofibroma and schwannoma. Curr Opin Neurol. 2002;15(6):679-84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
