

A pooled analysis evaluating prognostic significance of Residual Cancer Burden in invasive lobular breast cancer
- PMID: 39948079
- PMCID: PMC11825822
- DOI: 10.1038/s41523-025-00720-3
A pooled analysis evaluating prognostic significance of Residual Cancer Burden in invasive lobular breast cancer
Abstract
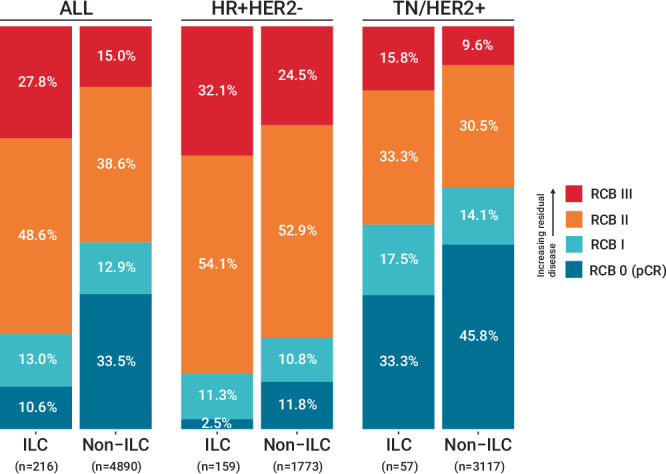
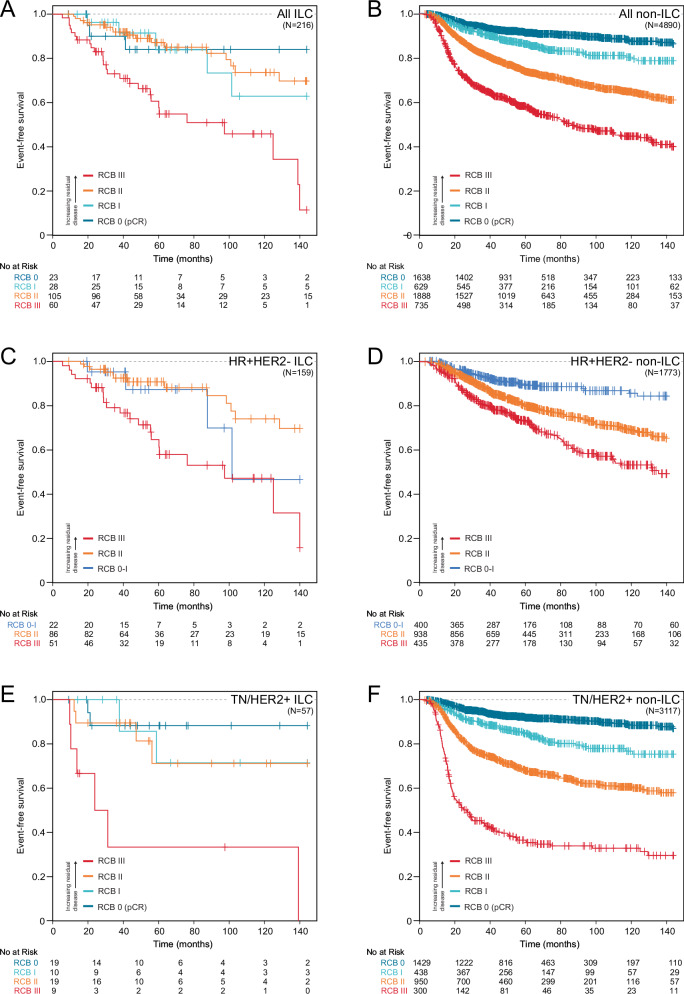
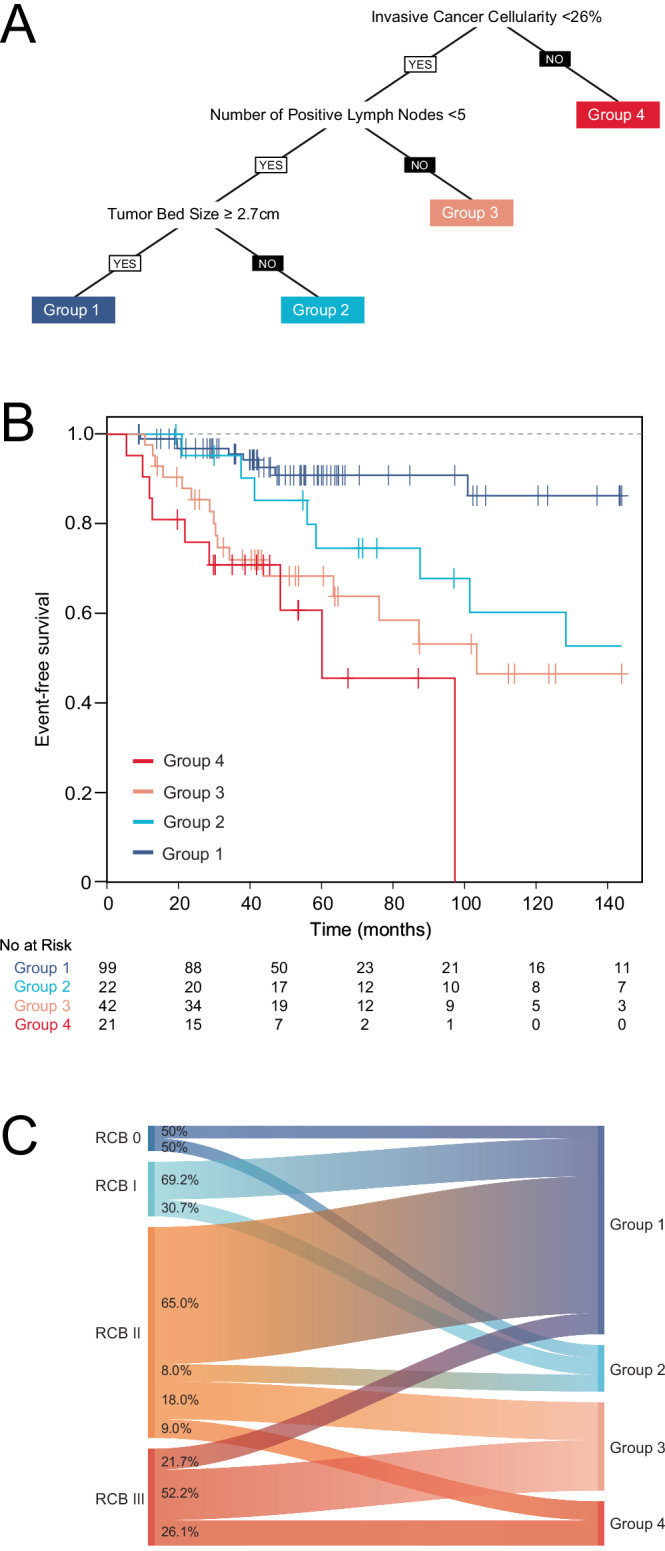
Residual Cancer Burden (RCB) after neoadjuvant chemotherapy (NAC) is validated to predict event-free survival (EFS) in breast cancer but has not been studied for invasive lobular carcinoma (ILC). We studied patient-level data from a pooled cohort across 12 institutions. Associations between RCB index, class, and EFS were assessed in ILC and non-ILC with mixed effect Cox models and multivariable analyses. Recursive partitioning was used in an exploratory model to stratify prognosis by RCB components. Of 5106 patients, the diagnosis was ILC in 216 and non-ILC in 4890. Increased RCB index was associated with worse EFS in both ILC and non-ILC (p = 0.002 and p < 0.001, respectively) and remained prognostic when stratified by receptor subtype and adjusted for age, grade, T category, and nodal status. Recursive partitioning demonstrated residual invasive cancer cellularity as most prognostic in ILC. These results underscore the utility of RCB for evaluating NAC response in those with ILC.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: RM reports research grant from GE Healthcare. CY reports institutional research funding from Quantum Leap Healthcare Collaborative. SLT reports consulting fees from AstraZeneca, Novartis, Roche, Pfizer, Celgene, Pierre-Fabre, Eisai, and Eli Lilly; reports honoraria from Eli Lilly; and reports travel support from Novartis, Celgene, Merck Sharp & Dohme, Roche, and Pfizer. HE reports institutional research funding from Roche Sanofi-Aventis; is a consultant for Daiichi-Sankyo, AstraZeneca, Intas Pharmaceuticals, and prIME Oncology; and reports travel support from Daiichi-Sankyo, AstraZeneca, Intas Pharmaceuticals, Pfizer, and Amgen. LH reports individual research grants from Roche and Sanofi-Aventis; and travel support from Roche, AstraZeneca, Pfizer, and Sanofi-Aventis. GSS reports institutional research funding from AstraZeneca, Merck, Novartis, and Roche. MM reports grants from Roche, Puma, and Novartis; is a consultant for AstraZeneca, Amgen, Glaxo, Taiho Oncology, Roche, Novartis, PharmaMar, Eli Lilly, Puma Biotechnology, Daiichi Sankyo, and Pfizer; reports honoraria from AstraZeneca, Amgen, Roche, Novartis, and Pfizer; and reports personal fees from Pfizer and Eli Lilly. JCB reports institutional funding from Eli Lilly and SymBioSis; participation on the Data Safety Monitoring Committee of Cairn Surgical; and has received honoraria from PER, PeerView, OncLive, EndoMag and Up-To-Date. MPG reports individual research grants from Pfizer, Sermonix, and Eli Lilly; and is a consultant for Pfizer, Eli Lilly, Novartis, Biotheranostics, Sermonix, Context Therapeutics, and Eagle Therapeutics. SBE reports institutional research funding from Pfizer. JEB reports institutional research funding from AstraZeneca; and honoraria from Pfizer and Eisai. JMSB reports grants from Thermo Fisher Scientific, Geoptix, Agendia, NanoString Technologies, Stratifyer, and Biotheranostics; is a consultant for Insight Genetics, BioNTech, Biotheranostics, Pfizer, RNA Diagnostics, and OncoXchange; reports honoraria from NanoString Technology, Oncology Education, and Biotheranostics; reports travel support from Biotheranostics and Nanostring Technologies; reports patents “histone gene module predicts anthracycline benefit” (Patent Cooperation Treaty [PCT] number CA2016/000247); “95-gene signature of residual risk following endocrine treatment” (PCT number CA2016/000304); “immune gene signature predicts anthracycline benefit” (PCT number CA2016/000305); and applied for patents “methods and devices for predicting anthracycline treatment efficacy” (USPTO application number 15/325,472; European Patent Office number 15822898.1; Canada, not yet assigned) and “systems, devices and methods for constructing and using a biomarker” (USPTO application number 15/328,108; European Patent Office number 15824751.0; Canada, not yet assigned). CC reports institutional funding from Genentech, Roche, Servier, and AstraZeneca; and participation in a data and safety monitoring advisory board for iMED External Science Panel. PH reports institutional research funding from Lilly, Eisai, Novartis, Merck, Gilead, Sanofi, Roche, Astrazeneca, Novartis, Abbvie and SeaGen. AKG reports personal fees from Sinochips Diagnostics. PS reports institutional research funding from Novartis, Merck, and Bristol Myers Squibb and Gilead; and is a consultant for Merck, Novartis, pfizer, Gilead, AstraZeneca, and ExactSciences. ADM reports institutional research funding from Novartis, Pfizer, Genentech and Neogenomics; Program Chair, Scientific Advisory Committee, ASCO. LP is a consultant for and receives honoraria from AstraZeneca, Merck, Novartis, Genentech, Eisai, Pieris, Immunomedics, Seattle Genetics, Almac, H3 Biomedicine, Clovis, and Syndax; and reports the patent “method of measuring residual cancer and predicting patient survival” (US Patent Number 7711494B2). LJvV is an employee of and owns stock in Agendia. DC reports institutional research funding from Novartis, AstraZeneca, Pfizer, Roche, Eli-Lilly, Puma Biotechnology, Daiichi Sankyo, Synthon, Seagen, Zymeworks, Elsevier, European Cancer Organisation, Celgene, Succinct Medical Communications, Prima BioMed (now Immutep), Oncolytics Biotech (US), Celldex Therapeutics, San Antonio Breast Cancer Consortium, Highfield Communication, Samsung Bioepis, prIME Oncology, Merck Sharp & Dohme, Prima BioMed (now Immutep), RTI Health Solutions, and Eisai. LJE reports institutional research funding from Merck; participation in an advisory board for Blue Cross Blue Shield; personal fees from UpToDate; and is an unpaid board member of Quantum Leap Healthcare Collaborative. WFS owns stocks in Delphi Diagnostics; and reports the patent “method of measuring residual cancer and predicting patient survival” (US Patent and Trademark Office [USPTO] number 7711494B2). All other authors declare no competing interests.
Figures

References
-
- Rastogi, P. et al. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project protocols B-18 and B-27. JCO26, 778–785 (2008). - PubMed
-
- Masuda, N. et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N. Engl. J. Med.376, 2147–2159 (2017). - PubMed
-
- von Minckwitz, G. et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N. Engl. J. Med.380, 617–628 (2019). - PubMed
-
- Cortazar, P. et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet384, 164–172 (2014). - PubMed
-
- Symmans, W. F. et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J. Clin. Oncol.25, 4414–4422 (2007). - PubMed
