

Intraoperative hemodynamic management in abdominal aortic surgery guided by the Hypotension Prediction Index: the Hemas multicentric observational study
- PMID: 39948674
- PMCID: PMC11823129
- DOI: 10.1186/s44158-024-00222-x
Intraoperative hemodynamic management in abdominal aortic surgery guided by the Hypotension Prediction Index: the Hemas multicentric observational study
Abstract
Background: Intraoperative hypotension (IOH) during non-cardiac surgery is closely associated with postoperative complications. Hypotensive events are more likely during major open vascular surgery. We prospectively investigated whether our institutional algorithm of cardiocirculatory management, which included the Hypotension Prediction Index (HPI), a predictive model of hypotension of the Hemosphere™ platform (Edwards Lifescience, Irwin, CA, USA), was able to reduce the incidence and severity of intraoperative hypotension during open abdominal aortic aneurysm repair.
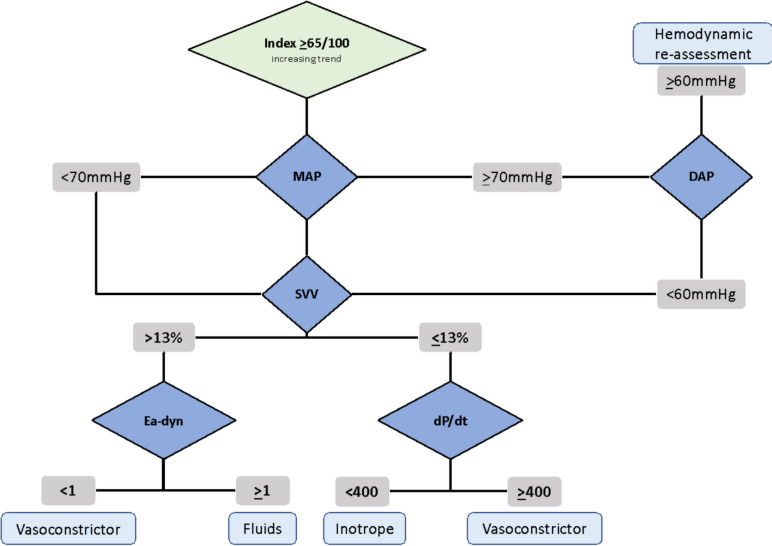
Methods: A multi-center observational study was conducted at IRCCS-Humanitas Research Hospital (Milan) and AO Mauriziano Umberto I Hospital (Turin) between July 2022 and September 2023, enrolling patients undergoing elective open abdominal aortic aneurysm repair. A hemodynamic protocol based on the Acumen-HPI Hemosphere™ platform was employed, integrating advanced parameters (e.g., HPI, Ea-dyn, dP/dt) and tailored interventions to minimize intraoperative hypotension. The primary endpoint was cumulative intraoperative hypotension time < 10% of surgical time, with secondary endpoints including incidence of hypotensive events, time-weighted averages of MAP < 65 mmHg (TWA65) and < 50 mmHg (TWA50), and postoperative complications.
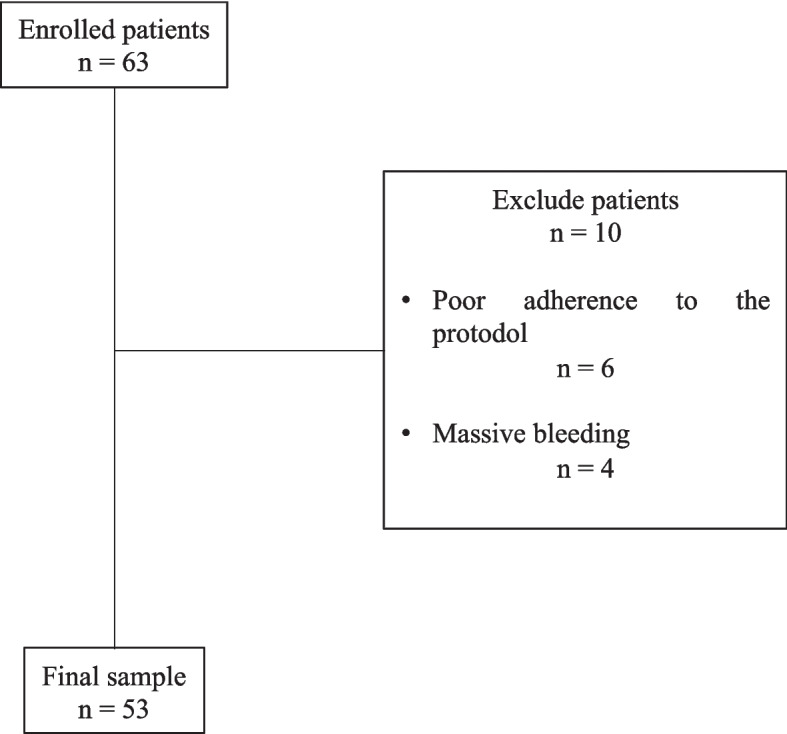
Results: We enrolled 53 patients submitted to open abdominal aortic repair. The primary endpoint (time in hypotension < 10%) was successfully reached: 5 [1-10] %. The targeted time-weighted average (< 0.40 mmHg) both for MAP < 65 mmHg (TWA65) and MAP < 50 mmHg (severe hypotension; TWA50) were reached: TWA65 = 0.26 [0.04-0.65] mmHg and TWA50 = 0.00 [0.00-0.01].
Conclusions: Our hemodynamic management algorithm based on the HPI and other parameters of the Hemosphere™ platform was able to limit the incidence and severity of intraoperative hypotension during open abdominal aortic repair.
Trial registration: NCT05478564.
Keywords: Abdominal aorta; Hemodynamic monitoring; Intraoperative hypo-tension; Open aortic repair; Vascular surgery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The research protocol was reviewed and approved by the independent local Ethical Committee of the IRCCS Humanitas research hospital (Aut. n. 3236–19/07/2022) and was registered in ClinicalTrials.gov (NCT05478564). Informed consent was obtained from all subjects involved in the study. Confidentiality of participant information was maintained, and all data collected were anonymized to protect privacy. Consent for publication: All patient data were de-identified prior to being included in the study. Competing interests: F.P:, E.G., F.N. and M.C. have received funds from Edwards Lifesciences for teaching events. The other authors have no conflicts of interest to declare.
Figures
References
-
- Walsh M, Devereaux PJ, Garg AX, Kurz A, Turan A, Rodseth RN et al (2013) Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology 119(3):507–515. Available from: https://pubmed.ncbi.nlm.nih.gov/23835589/. Cited 2023 Oct 17 - PubMed
-
- Maheshwari K, Turan A, Mao G, Yang D, Niazi AK, Agarwal D et al (2018) The association of hypotension during non-cardiac surgery, before and after skin incision, with postoperative acute kidney injury: a retrospective cohort analysis. Anaesthesia 73(10):1223–1228. Available from: https://pubmed.ncbi.nlm.nih.gov/30144029/. Cited 2024 Oct 11 - PubMed
-
- Sun LY, Wijeysundera DN, Tait GA, Beattie WS (2015) Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology 123(3):515–523. Available from: (https://pubmed.ncbi.nlm.nih.gov/26181335/.). Cited 2024 Oct 11 - PubMed
-
- Bijker JB, Van Klei WA, Vergouwe Y, Eleveld DJ, Van Wolfswinkel L, Moons KGM et al (2009) Intraoperative hypotension and 1-year mortality after noncardiac surgery. Anesthesiology 111(6):1217–1226. Available from: https://pubmed.ncbi.nlm.nih.gov/19934864/. Cited 2024 Oct 11 - PubMed
-
- Salmasi V, Maheshwari K, Yang D, Mascha EJ, Singh A, Sessler DI et al (2017) Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: a retrospective cohort analysis. Anesthesiology 126(1):47–65. Available from: https://pubmed.ncbi.nlm.nih.gov/27792044/. Cited 2024 Oct 11 - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical