

Cold Ceramic for Repairing Root Perforations: A Case Report
- PMID: 39949583
- PMCID: PMC11821458
- DOI: 10.1002/ccr3.70182
Cold Ceramic for Repairing Root Perforations: A Case Report
Abstract
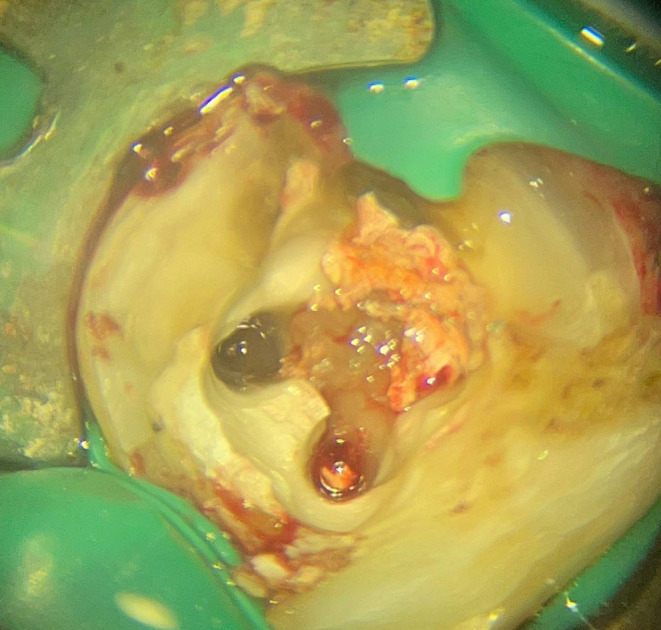
Root perforation may happen pathologically or iatrogenically at any stage of endodontic treatment. Repairing a Perforation can be challenging and can negatively affect the prognosis of the treatment. The prognosis depends on various factors, including the size and site of the perforation, the presence of microorganisms, and the time lapse between injury and repair. One crucial factor is using a suitable material with favorable biocompatibility, moisture tolerance, and sealing abilities. Thus, choosing the suitable perforation sealing material can significantly affect the outcomes. Many materials have been suggested for perforation repair. However, searching for an ideal material continues, indicating the complicated nature of root perforations. In this study, three patients, two male and one female, received treatment for root perforation, each varying in the prognosis determinant factors. All cases were managed non-surgically with cold ceramic (CC) as the repairing material. After follow-up, they were clinically and radiographically examined, and all three cases revealed relatively complete healing of the tissues and no signs or symptoms of inflammation. The results obtained from the presented cases indicated CC's sealing ability, biocompatibility, moisture tolerance, and bone and periodontium regeneration, which are essential for successful perforation repair. The favorable healing of the perforation and the elimination of inflammation in every case, as well as the existing literature, support the use of CC as a suitable material for sealing perforations. However, additional clinical research is recommended to further understand CC's qualities and potential.
Keywords: MTA; case report; cold ceramic; retreatment; root canal therapy; root filling material.
© 2025 The Author(s). Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







































References
-
- Clauder T., “Repair of Pulp Chamber and Root Perforations,” in Endodontic Advances and Evidence‐Based Clinical Guidelines (Wiley, 2022), 475–510.
-
- Thamilselvan A. and Ramesh S., “Clinical Practice Guidelines for the Management of Endodontic Perforation,” Journal of Pharmacological Research 12 (2020): 4046–4053, 10.31838/ijpr/2020.SP2.501. - DOI
LinkOut - more resources
Full Text Sources
