

Local tumor control and neurological outcomes after surgery for spinal hemangioblastomas in sporadic and von Hippel-Lindau disease: A multicenter study
- PMID: 39950840
- PMCID: PMC12309710
- DOI: 10.1093/neuonc/noaf041
Local tumor control and neurological outcomes after surgery for spinal hemangioblastomas in sporadic and von Hippel-Lindau disease: A multicenter study
Abstract
Background: Spinal hemangioblastomas (sHBs) are rare vascular tumors with significant neurological implications. Their management, particularly in von Hippel-Lindau (VHL) disease, remains challenging due to recurrence and functional decline. Timely identification and intervention are critical for optimal outcomes.
Methods: This international, multicenter retrospective cohort study included 357 patients (199 VHL-associated, 158 sporadic) from 13 neuro-oncological centers. Clinical and imaging data were analyzed to assess progression-free survival (PFS) and functional outcomes using the modified McCormick Scale (mMCS) at 12 months. Secondary analyses identified factors associated with VHL disease in sHBs.
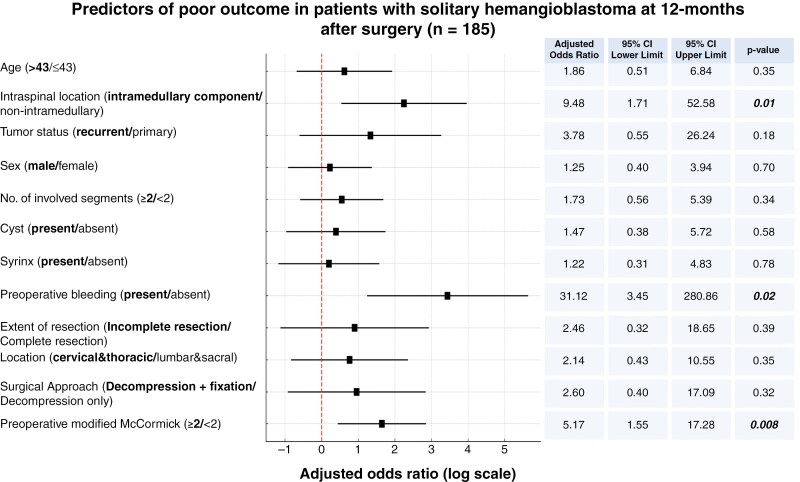
Results: Complete resection was achieved in 87.7% of cases, leading to significantly improved PFS at 72 months (sporadic: 95.1%, VHL-associated: 91.1%; hazard ratio: 0.18, 95% CI: 0.08-0.4). Multivariable analysis identified predictors of unfavorable outcomes at 12 months: preoperative mMCS ≥2 (odds ratio [OR]: 5.17, P = .008), intramedullary tumor location (OR: 9.48, P = .01), and preoperative bleeding (OR: 31.12, P = .02). Factors independently associated with VHL disease in sHBs included non-cervical tumor location (OR: 2.08, P = .004), intramedullary growth (OR: 2.39, P < .001), and age <43 years (OR: 3.24, P < .001). Functional improvements were observed in most patients, particularly those with sporadic sHBs.
Conclusions: Complete surgical resection is essential for long-term tumor control and favorable functional outcomes in both sporadic and VHL-associated sHBs. Early intervention, particularly in mild symptomatic and progressive cases, before neurological deterioration or hemorrhage, optimizes recovery. This study, the largest of its kind in a multicentric international setting, provides robust evidence to guide the management of both sporadic and VHL-associated sHBs.
Keywords: complete resection; multicenter study; neurological outcomes; progression-free survival; spinal hemangioblastomas; von Hippel–Lindau disease.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Conflict of interest statement
B.M.—Grants: Zeiss (Institution), Brainlab (Institution), Sonovum (Institution); Royalties: Medacta (Personal), Spineart (Personal), Icotec (Personal); Consulting: Medacta, Brainlab, Zeiss, Icotec (Personal); Support for travel: Brainlab, Zeiss, Icotec, Medacta, Spineart (Payments for meetings and travel); Stock: Sonovum. S.K.—Consulting: Brainlab, Ulrich Medical, Need Inc.; Honoraria: Brainlab (Lectures); Support for travel: Nexstim Plc. L.R.—Grants: German Ministry of Education and Research (BMBF), GoBio Program, European Association of Neurosurgical Societies (EANS), Research Fund Program. V.M.B.—Consulting: Brainlab. J.W.—Honoraria: Novocure (Lectures); Support for travel: Carl Zeiss, Stryker (Meetings and travel). C.T.—Consulting: Carl Zeiss, Stryker (Advisory Board); Honoraria: Carl Zeiss, Stryker (Lectures). F.K.—Support for travel: Carl Zeiss, Stryker (Meetings and travel). Authors not listed have nothing to disclose.
Figures




References
-
- Deng X, Wang K, Wu L, et al. Intraspinal hemangioblastomas: analysis of 92 cases in a single institution: clinical article. J Neurosurg Spine. 2014;21(2):260–269. - PubMed
-
- Glenn GM, Linehan WM, Hosoe S, et al. Screening for von Hippel-Lindau disease by DNA polymorphism analysis. JAMA. 1992;267(9):1226–1231. - PubMed
-
- Lonser RR. Surgical management of sporadic spinal cord hemangioblastomas. World Neurosurg. 2014;82(5):632–633. - PubMed
-
- Yousef A, Rutkowski MJ, Yalcin CE, et al. Sporadic and Von-Hippel Lindau disease-associated spinal hemangioblastomas: institutional experience on their similarities and differences. J Neurooncol. 2019;143(3):547–552. - PubMed
-
- Conway JE, Chou D, Clatterbuck RE, et al. Hemangioblastomas of the central nervous system in von Hippel-Lindau syndrome and sporadic disease. Neurosurgery. 2001;48(1):55–62; discussion 62–63. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
