

Phase 1 trial of durvalumab (anti-PD-L1) combined with lenalidomide in relapsed/refractory cutaneous T-cell lymphoma
- PMID: 39951620
- PMCID: PMC12088755
- DOI: 10.1182/bloodadvances.2024014655
Phase 1 trial of durvalumab (anti-PD-L1) combined with lenalidomide in relapsed/refractory cutaneous T-cell lymphoma
Abstract
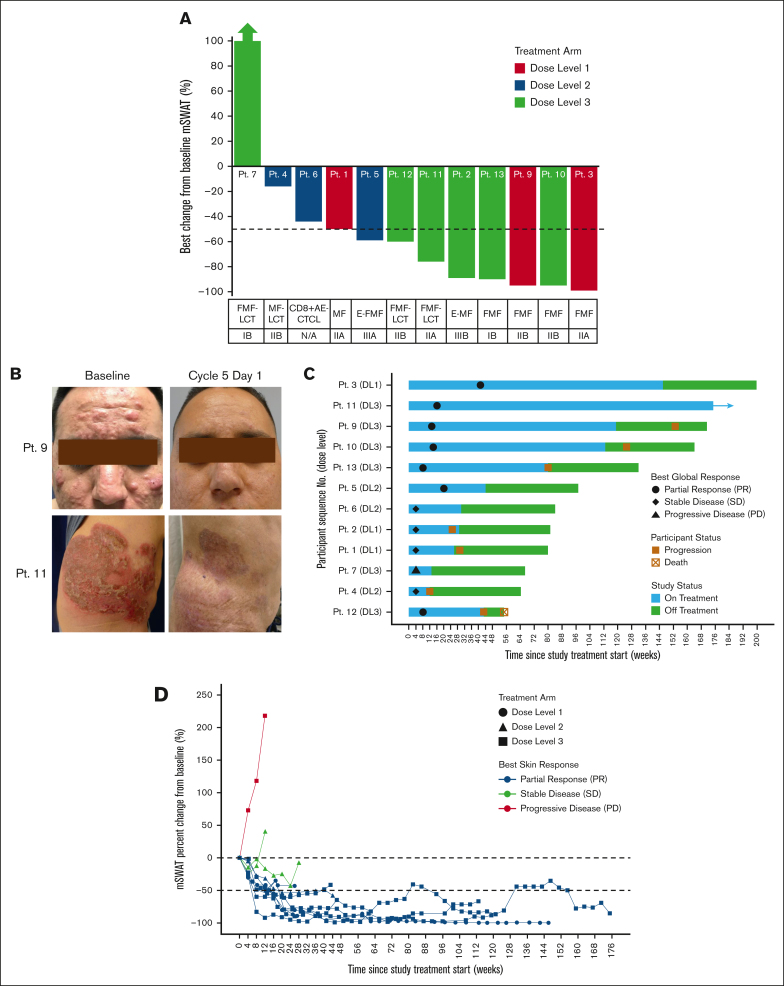
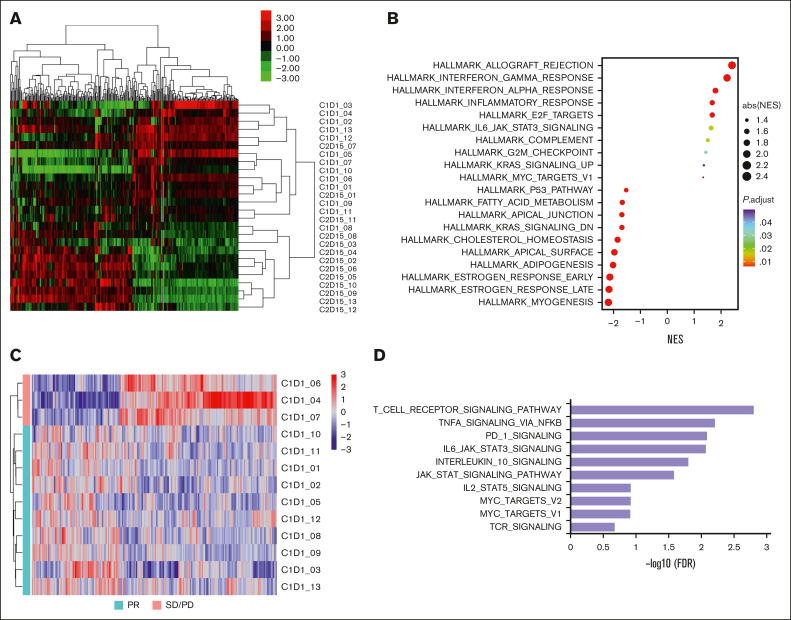
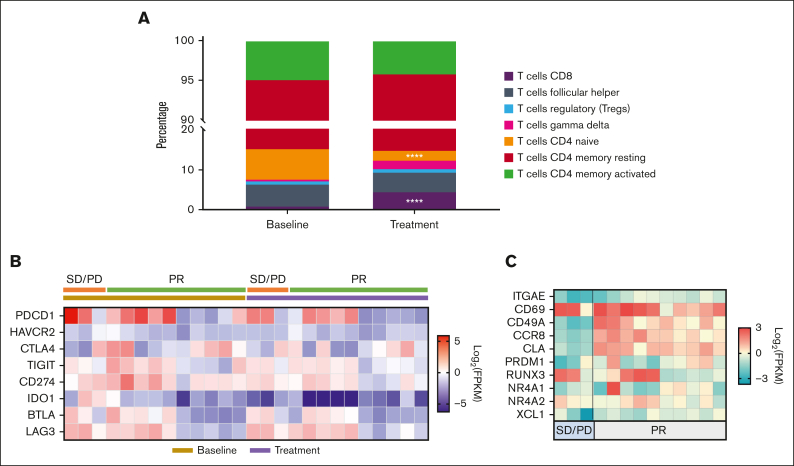
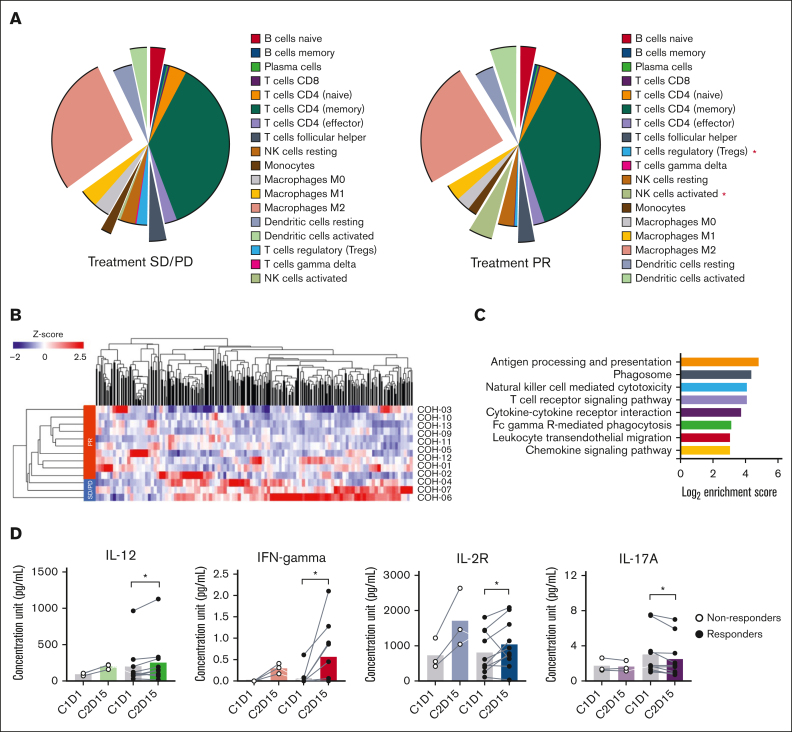
Selective targeting of the functionally exhausted malignant T cells in cutaneous T-cell lymphoma (CTCL) and distinct cells within the tumor microenvironment (TME) via programmed cell death 1/programmed cell death ligand 1 blockade (durvalumab) may restore an antitumor immune response. The oral immunomodulator lenalidomide, which has activity in CTCL, may enhance durvalumab immune checkpoint blockade. Our phase 1/2 clinical trial of durvalumab and lenalidomide in patients with refractory/advanced CTCL sought to assess the safety and tolerability and to identify the maximum tolerated dose and recommended phase 2 dose (RP2D) of lenalidomide plus fixed-dose durvalumab. Secondary and tertiary objectives were to investigate the efficacy and effects on the TME. Thirteen patients were evaluable for toxicities and 12 for dose decisions and response. No serious adverse events (AEs) or dose-limiting toxicities (DLTs) were observed during cycles 1 to 3 (DLT evaluation period), and dose level 3 was identified as the RP2D. The most frequent AEs were tumor flare, fatigue, neutropenia, and leukopenia. Three patients developed grade 1 or 2 autoimmune thyroiditis that resolved with treatment. Best overall and skin response rates were 58.3% (95% confidence interval (95% CI), 27.7-84.8%) and 75% (95% CI: 42.8-94.5%), respectively. The median cycles of treatment were 11, and the median duration of response was 25.5 months. The combination showed clinical activity with 7 partial responses and 4 stable disease. Potentially predictive immune signatures were downregulation of -α signaling via NF-κB, interferon gamma, and phosphoinositide 3 kinase-AKT-mammalian target of rapamycin signaling pathways in responders and upregulation of MYC targets and proinflammatory pathways in nonresponders. Profiling of immune cell compositions revealed changes in individual immune cell clusters based on treatment response. This trial was registered at www.ClinicalTrials.gov as #NCT03011814.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: C.Q. reports research grants from Celgene, Helsinn, and Kyowa Kirin; serving as a clinical investigator for Kyowa Kirin, SIRPant, and BioInvent; and serving on advisory boards or steering committees for Helsinn, Kyowa Kirin, and Citius Pharmaceuticals. J.Z. reports serving on the speakers bureau for Kyowa Kirin, and research/grant support from Seattle Genetics, Daiichi Sankyo, Dreon, Myeloid Therapeutics, CRISPR, and Astrix. The remaining authors declare no competing financial interests.
Figures

References
-
- Agar NS, Wedgeworth E, Crichton S, et al. Survival outcomes and prognostic factors in mycosis fungoides/Sezary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. J Clin Oncol. 2010;28(31):4730–4739. - PubMed
-
- Arulogun SO, Prince HM, Ng J, et al. Long-term outcomes of patients with advanced-stage cutaneous T-cell lymphoma and large cell transformation. Blood. 2008;112(8):3082–3087. - PubMed
-
- Guenova E, Hoetzenecker W, Rozati S, Levesque MP, Dummer R, Cozzio A. Novel therapies for cutaneous T-cell lymphoma: what does the future hold? Expert Opin Investig Drugs. 2014;23(4):457–467. - PubMed
-
- Hughes CF, Khot A, McCormack C, et al. Lack of durable disease control with chemotherapy for mycosis fungoides and Sezary syndrome: a comparative study of systemic therapy. Blood. 2015;125(1):71–81. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
