

Predictors of futile recanalization after intravenous thrombolysis in stroke patients transferred for endovascular treatment
- PMID: 39954040
- PMCID: PMC11885372
- DOI: 10.1007/s11239-025-03070-w
Predictors of futile recanalization after intravenous thrombolysis in stroke patients transferred for endovascular treatment
Abstract
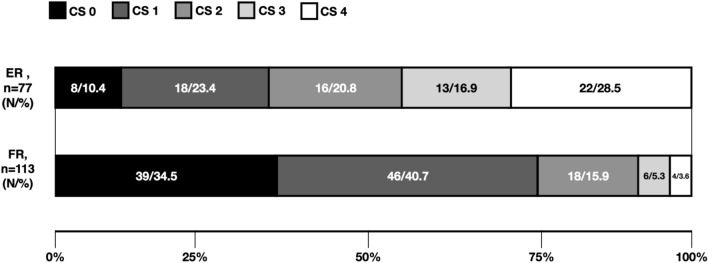
Some patients with large vessel occlusion (LVO) achieve insufficient clinical improvement (futile recanalization, FR) after intravenous thrombolysis (IVT) during inter-hospital transfer for thrombectomy, while others show good outcomes (effective recanalization, ER). This study assessed FR and ER rates among patients treated with IVT at non-thrombectomy primary stroke centers (PSCs) and aimed to identify predictors of FR. We analyzed data from two PSC registries (2016-2022). Inclusion criteria: IVT treatment, anterior circulation LVO, NIHSS ≥ 6, ASPECTS ≥ 5, and documented recanalization at thrombectomy centers. FR was defined as a 90-day poor outcome (mRS 3-6) despite LVO recanalization on initial angiography. Among 190 PSC patients with documented recanalization post-IVT, 113 (59.5%) had FR. Multivariable analysis identified age (OR = 1.03, 95%CI = 1.01-1.07, p = 0.021), NIHSS at the PSC (OR = 1.13, 95%CI = 1.05-1.22, p = 0.026), and collateral status (OR = 0.54, 95%CI = 0.39-0.75, p = 0.001) as independent predictors of FR and 90-day mortality. A model combining age, NIHSS, and collateral score provided the highest predictive accuracy for FR and mortality. FR is common in LVO-related ischemic stroke treated with IVT at non-thrombectomy centers. FR is common in LVO-related ischemic stroke treated with IVT at non-thrombectomy centers. Identifying predictors of FR can guide clinicians in early decision-making, allowing for tailored interventions and informed discussions about expected outcomes, potentially leading to more optimized patient management.The GOTIC-VTE trial Unique identifier, jRCTs031180124; Registration date, April 06, 2017.
Keywords: Collateral circulation; Futile recanalization; Hub; Intravenous thrombolysis; Mechanical thrombectomy; Spoke.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: SB is a key opinion leader for RAPIDAI. All other authors have no conflicts of interests. Ethical approval: This study has obtained approval from the UK Health Regulator Authority (HRA) (HRA Reference No.: 275260). The study has also received confirmation of capacity and capability from the Imperial College Healthcare NHS Trust. Informed consent: Informed consent was not a legal requirement as the research was carried out using data collected as part of routine care and any researchers outside the direct care team only had access to anonymized data.
Figures


References
-
- Powers WJ, Rabinstein AA, Ackerson T, Guidelines for the Early Management of Patients With Acute Ischemic Stroke, et al (2019) Update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 10.1161/STR.0000000000000211 - PubMed
-
- Espinosa de Rueda M, Parrilla G, Manzano-Fernández S et al (2015) Combined multimodal computed tomography score correlates with futile recanalization after thrombectomy in patients with acute stroke. Stroke 46:2517–2522 - PubMed
-
- Goyal M, Menon BK, van Zwam WH et al (2016) Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. The Lancet 387:1723–1731 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
