

Exploring high-throughput drug sensitivity testing in neuroblastoma cell lines and patient-derived tumor organoids in the era of precision medicine
- PMID: 39954414
- PMCID: PMC11884408
- DOI: 10.1016/j.ejca.2025.115275
Exploring high-throughput drug sensitivity testing in neuroblastoma cell lines and patient-derived tumor organoids in the era of precision medicine
Abstract
Introduction: Despite druggable events to be present in 80 % of neuroblastomapatients within the Princess Máxima Center precision medicine program 'iTHER', clinical uptake of treatment recommendations has been low, and the clinical impact for individual patients remains hard to predict. This stresses the need for a method integrating genomics and transcriptomics with functional approaches into therapeutic decision making.
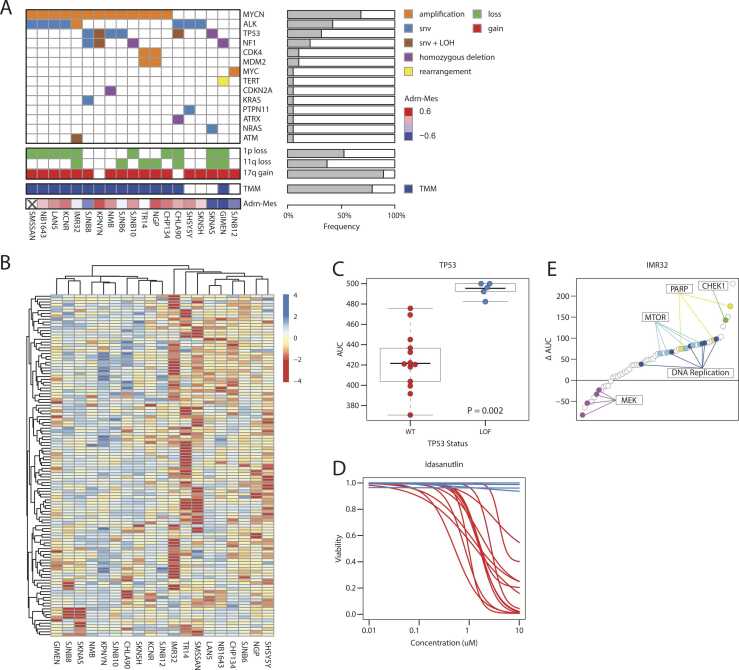
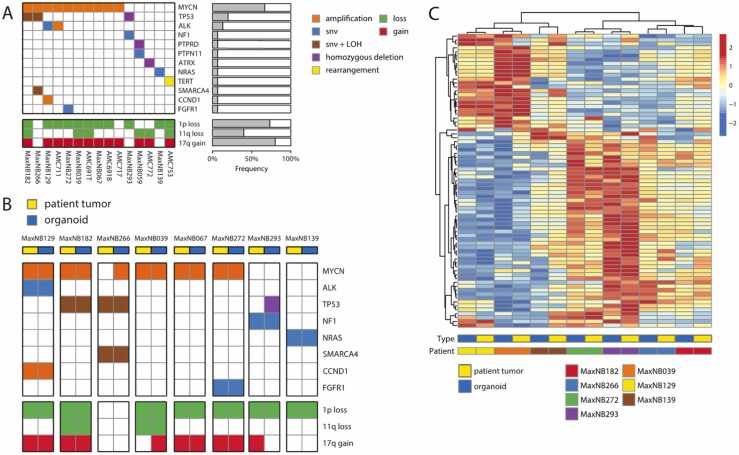
Methods: We aimed to launch an online repository integrating genomics and transcriptomics with high-throughput drug screening (HTS) of nineteen commonly used neuroblastoma cell lines and fifteen neuroblastoma patient-derived organoids (NBL-PDOs). Cell lines, NBL-PDOs and their parental tumors were characterized utilizing (lc)WGS, WES and RNAseq. Cells were exposed to ∼200 compounds. Results were transferred to the R2 visualization platform.
Results: A powerful reference set of cell lines is available, reflecting distinct known pharmacologic vulnerabilities. HTS identified additional therapeutic vulnerabilities, such as a striking correlation between a positive mesenchymal signature and sensitivity to BCL2-inhibitor venetoclax. Finally, we explored personalized drug sensitivities within iTHER, demonstrating HTS can support genomic and transcriptomic results, thereby strengthening the rationale for clinical uptake.
Conclusion: We established a dynamic publicly available dataset with detailed genomic, transcriptomic, and pharmacological annotation of classical neuroblastoma cell lines as well as novel sharable NBL-PDOs, representing the heterogeneous landscape of neuroblastoma. We anticipate that in vitro drug screening will be complementary to genomic-guided precision medicine by supporting clinical decision making, thereby improving prognosis for all neuroblastoma patients in the future.
Keywords: Adolescent; Cancer; Child; High-throughput drug screening; Molecular biology; Molecular targeted therapy; Neuroblastoma; Next-generation sequencing; Organoid; Precision medicine.
Copyright © 2025 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Moreno L., Rubie H., Varo A., Le Deley M.C., Amoroso L., Chevance A., et al. Outcome of children with relapsed or refractory neuroblastoma: a meta-analysis of ITCC/SIOPEN European phase II clinical trials. Pediatr Blood Cancer. 2017;64:25–31. - PubMed
-
- London W.B., Bagatell R., Weigel B.J., Fox E., Guo D., Van Ryn C., et al. Historical time to disease progression and progression-free survival in patients with recurrent/refractory neuroblastoma treated in the modern era on Children's Oncology Group early-phase trials. Cancer. 2017;123:4914–4923. - PMC - PubMed
-
- Allemani C., Matsuda T., Di Carlo V., Harewood R., Matz M., Niksic M., et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391:1023–1075. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
