

Optimizing nutritional strategies in term NEC and perforation infants after intestinal operation: a retrospective study
- PMID: 39955353
- PMCID: PMC11829962
- DOI: 10.1038/s41598-025-90366-9
Optimizing nutritional strategies in term NEC and perforation infants after intestinal operation: a retrospective study
Abstract
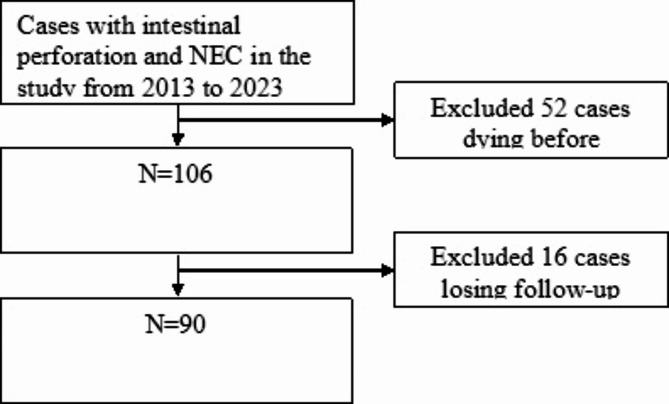
Necrotizing enterocolitis (NEC) represents a severe condition in infants, with perforation being a particularly critical pathological manifestation. However, there is an absence of guidelines regarding the refeeding of infants recovering from perforation subsequent to NEC. This study aimed to determine the optimal refeeding method for term infants recovering from perforation after NEC. The study encompassed three aspects: the timing of enteral nutrition (EN) resumption, the progression of EN, and the method of EN resumption. Ninety full-term neonates who developed perforation following NEC and underwent surgical intervention were included. These samples were divided into early enteral nutrition (EEN, < 7 days) and late enteral nutrition (LEN, ≥ 7 days) groups based on the timing of EN resumption; faster increase (FI, ≥ 20 ml/kg/d) and slower increase (SI, < 20 ml/kg/d) groups based on the progression of EN; intact protein formula (IPF), special medical formula (SMF, including EHF and AABF), and mixed feeding (MF) groups based on the method of EN resumption. EEN infants had a lower incidence of intestinal stenosis and reoperation (43.5% vs. 77.6%, p = 0.002; 60.9% vs. 82.1%, p = 0.038), and a shorter duration of hospital stay after surgery and parenteral nutrition (PN) than LEN infants (14 days vs. 20 days, p < 0.001; 11 days vs. 17 days, p < 0.001). Faster increasing feed volumes was associated with shorter duration of hospital stay and parenteral nutrition (15 days vs. 20 days, p < 0.001; 14 days vs. 17 days, p < 0.001), but a slower rate of weight gain (0.020 kg vs. 0.129 kg, p < 0.01). The time to repeat NPO in SMF group is shorter than IPF an MF groups (3 days vs. 4 days and 9 days, p = 0.025). Our study demonstrates the beneficial effects of early enteral feeding and fast advancement of feed volumes in term infants with NEC and perforation after surgery, specifically in reducing short-term complications and the duration of hospital stay following surgery and PN. Additionally, this study suggests that IPF and MF significantly contribute to stimulate intestinal adoption recovery.
Keywords: Intestinal perforation; Intestinal resection; Intestinal stenosis; Necrotizing enterocolitis; Nutrition; Term infants.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
References
-
- Zani, A. et al. International survey on the management of necrotizing enterocolitis. Eur. J. Pediatr. Surg. Off J. Austrian Assoc. Pediatr. Surg. Al Z. Kinderchir. 25 (1), 27–33 (2015). - PubMed
-
- Bohnhorst, B. et al. Early feeding after necrotizing enterocolitis in preterm infants. J. Pediatr.143 (4), 484–487 (2003). - PubMed
-
- Han, S. M. et al. Trends in incidence and outcomes of necrotizing enterocolitis over the last 12 years: a multicenter cohort analysis. J. Pediatr. Surg.55 (6), 998–1001 (2020). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
