

How low can we go? The effect of acquisition duration on cardiac volume and function measurements in free-running cardiac and respiratory motion-resolved five-dimensional whole-heart cine magnetic resonance imaging at 1.5T
- PMID: 39956514
- PMCID: PMC12019821
- DOI: 10.1016/j.jocmr.2025.101863
How low can we go? The effect of acquisition duration on cardiac volume and function measurements in free-running cardiac and respiratory motion-resolved five-dimensional whole-heart cine magnetic resonance imaging at 1.5T
Abstract
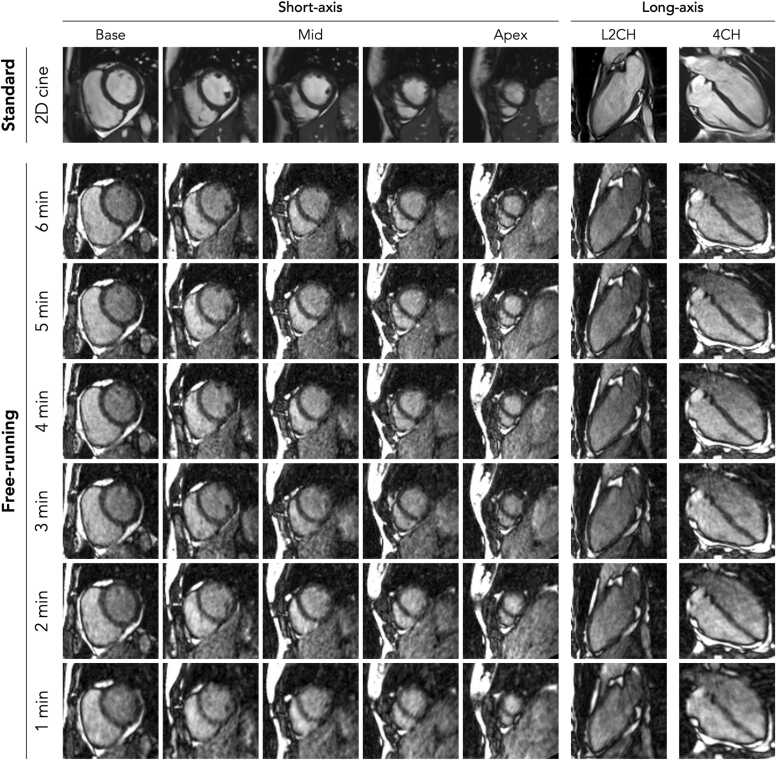
Background: Cardiovascular magnetic resonance (CMR) is the gold standard for assessing cardiac volumes and function using two-dimensional (2D) breath-held cine imaging. This technique, however, requires a reliable electrocardiogram (ECG) signal, repetitive breath-holds, and the time-consuming and proficiency-demanding planning of cardiac views. Recently, a free-running framework has been developed for cardiac and respiratory motion-resolved five-dimensional (5D) whole-heart imaging without the need for an ECG signal, repetitive breath-holds, and meticulous plan scanning. In this study, we investigate the impact of acquisition time on cardiac volumetric and functional measurements, when using free-running imaging, compared to reference standard 2D cine imaging.
Methods: Sixteen healthy adult volunteers underwent CMR at 1.5T, including standard 2D breath-held cine imaging and free-running imaging using acquisition durations ranging from 1 to 6 min in randomized order. All datasets were anonymized and analyzed for left-ventricular end-systolic volume (ESV) and end-diastolic volume (EDV), as well as ejection fraction (EF). In a subset of data, intra- and inter-observer agreement was assessed. In addition, image quality and observer confidence were scored using a 4-point Likert scale. Finally, acquisition efficiency was reported for both imaging techniques, which was defined as the time required for data sampling divided by the total scan time.
Results: No significant differences in left-ventricular EDV and ESV were found between free-running imaging for 1, 2, 3, 5, and 6 min and standard 2D breath-held cine imaging. Biases in EDV ranged from -2.4 to -7.4 mL, while biases in ESV ranged from -3.8 to 2.1 mL. No significant differences in EF were found between free-running imaging of any acquisition duration and standard 2D breath-held cine imaging. Biases in EF ranged from -2.8% to 0.94%. Both image quality and observer confidence in free-running imaging improved when the acquisition duration increased. However, they were always lower than standard 2D breath-held cine imaging. Acquisition efficiency improved from 13% for standard 2D cine imaging to 50% or higher for free-running imaging.
Conclusion: Free-running CMR with an acquisition duration as short as 1min can provide left-ventricular cardiac volumes and EF comparable to standard 2D breath-held cine imaging, albeit at the expense of both image quality and observer confidence.
Keywords: 5D; CMR; Cardiac MRI; Free-breathing; Free-running; Self-gating.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interests The authors declare the following financial interests/personal relationships which may be considered as potential competing interests. Robert J. Holtackers reports financial support was provided by Niels Stensen Fellowship. Ruud B. van Heeswijk, Christopher W. Roy, Jerome Yerly, and Matthias Stuber report financial support was provided by Swiss National Science Foundation. Ludovica Romanin reports a relationship with Siemens Healthcare that includes: employment. Matthias Stuber reports a relationship with Siemens Healthcare that includes non-financial support. Ruud B. Van Heeswijk is an associate editor of JCMR. Matthias Stuber is a senior advisor of JCMR. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
-
- Nussbaumer C., Bouchardy J., Blanche C., Piccini D., Pavon A.G., Monney P., et al. 2D cine vs. 3D self-navigated free-breathing high-resolution whole heart cardiovascular magnetic resonance for aortic root measurements in congenital heart disease. J Cardiovasc Magn Reson. 2021;23(1):65. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
