

Effect of restrictive fluid resuscitation on severe acute kidney injury in septic shock: a systematic review and meta-analysis
- PMID: 39956601
- PMCID: PMC11831265
- DOI: 10.1136/bmjopen-2024-086367
Effect of restrictive fluid resuscitation on severe acute kidney injury in septic shock: a systematic review and meta-analysis
Abstract
Objectives: Sepsis-associated hypotension or shock is a critical stage of sepsis, and a current clinical emergency that has high mortality and multiple complications. A new restrictive fluid resuscitation therapy has been applied, and its influence on patients' renal function remains unclear. The purpose of this study is to evaluate the influence of restrictive fluid resuscitation on incidence of severe acute kidney injury (AKI) in adult patients with sepsis hypotension and shock compared with usual care.
Design: Systematic review and meta-analysis using the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach.
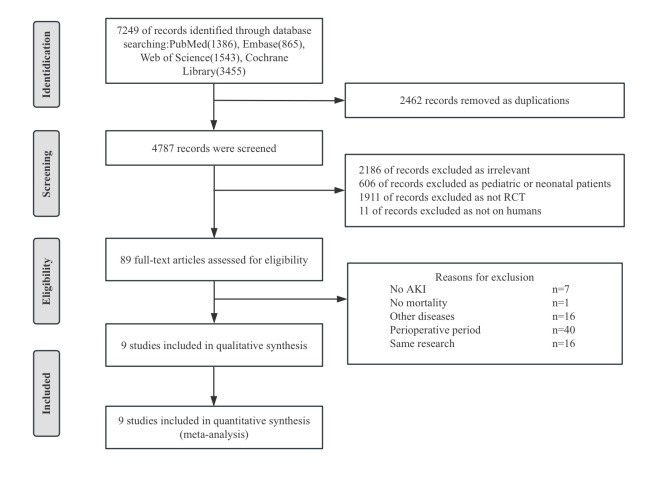
Data sources: PubMed, Embase, Web of Science and Cochrane Library were searched through 1 November 2024.
Eligibility criteria: We included randomised controlled trials that compared restrictive fluid resuscitation with liberal fluid therapy on patients with sepsis-associated hypotension and shock, to find out their effect on the incidence of severe AKI. Severe AKI was defined as the AKI network score 2-3 or Kidney Disease Improving Global Outcomes stages 2 and 3.
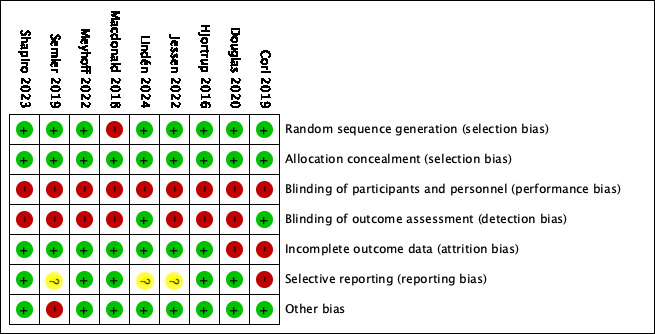
Data extraction and synthesis: Two independent reviewers used standardised methods to search, screen and code included trials. Risk of bias was assessed using the Cochrane Systematic Review Handbook for randomised clinical trials. Meta-analysis was conducted using random effects models. Sensitivity and subgroup analyses, trial sequential analysis (TSA), Egger's test and the trim-and-fill method were performed. Findings were summarised in GRADE evidence profiles and synthesised qualitatively.
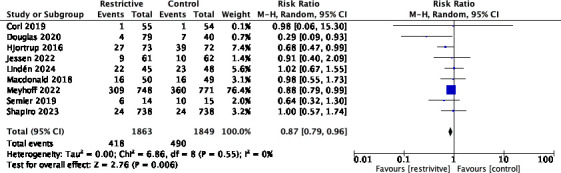
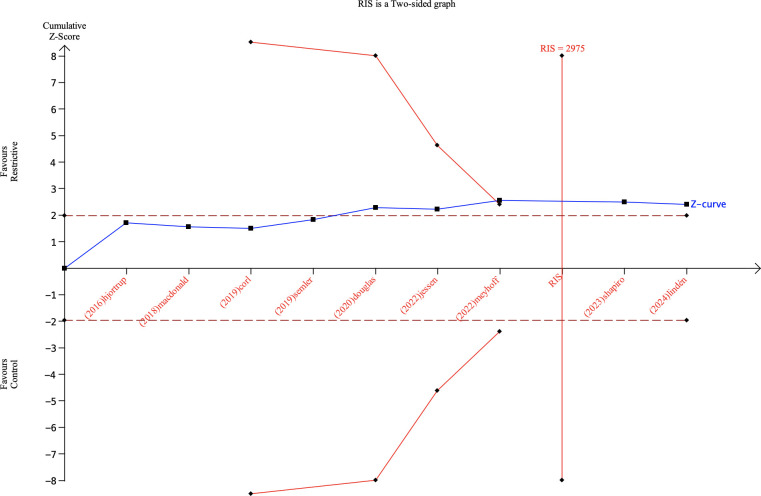
Results: Nine trials (3718 participants) were included in this research and the analysis was conducted in random effects model. There was a significant difference in the incidence of severe AKI (risk ratio 0.87, 95% CI 0.79 to 0.96, p=0.006; I2=0%) and the duration of mechanical ventilation (mean difference -41.14, 95% CI -68.80 to -13.48; p=0.004; I2=74%) between patients receiving restrictive fluid resuscitation and patients receiving liberal fluid resuscitation. TSA showed that the cumulative amount of participants met the required information size, the positive conclusion had been confirmed. The GRADE assessment results demonstrated moderate confidence in the incidence of severe AKI, as well as the results of all second outcomes except the Intensive Care Unit length of stay (ICU LOS), which received limited confidence. The result of incidence of worse AKI was rated as of high certainty.
Conclusions: It is conclusive that fluid restriction strategy is superior to usual care when it comes to reducing the incidence of severe AKI in sepsis-associated hypotension and shock. Shorter duration of ventilation is concerned with fluid restriction as well, but the heterogeneity is substantial. GRADE assessments confirmed moderate and above certainty. Traditional fluid resuscitation therapy has the potential to be further explored for improvements to be more precise and appropriate for a better prognosis.
Prospero registration number: CRD42023449239.
Keywords: Acute renal failure; Adult intensive & critical care; Mortality.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous