

Stress T1 mapping and quantitative perfusion cardiovascular magnetic resonance in patients with suspected obstructive coronary artery disease
- PMID: 39957254
- PMCID: PMC12123514
- DOI: 10.1093/ehjci/jeaf059
Stress T1 mapping and quantitative perfusion cardiovascular magnetic resonance in patients with suspected obstructive coronary artery disease
Abstract
Aims: T1 mapping reactivity (ΔT1) has been proposed as a novel contrast-free technique to detect obstructive coronary artery disease (CAD). The aims of the study are: (i) to compare the cardiovascular magnetic resonance (CMR)-derived ΔT1 with quantitative perfusion (QP CMR) measures; (ii) to assess the influence of sex and comorbidities on ΔT1; and (iii) to assess the diagnostic accuracy of ΔT1 to detect obstructive CAD diagnosed with the invasive coronary angiography (ICA) and/or fractional flow reserve.
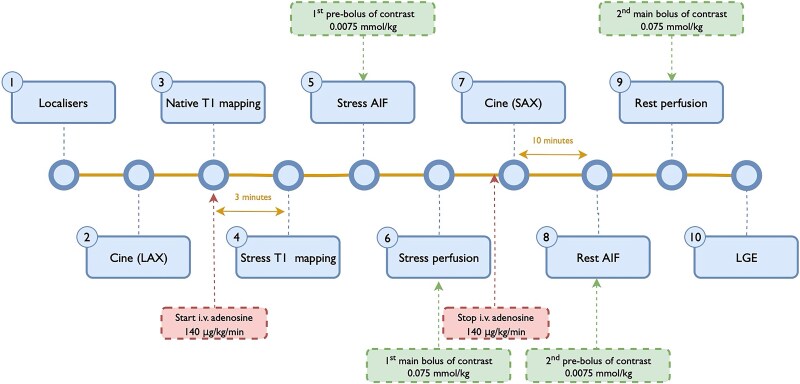
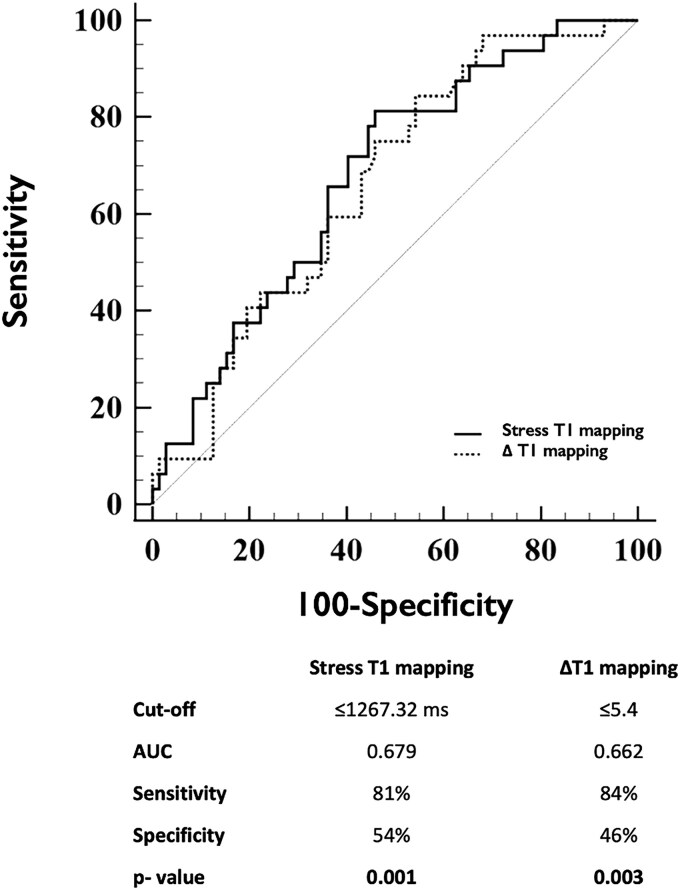
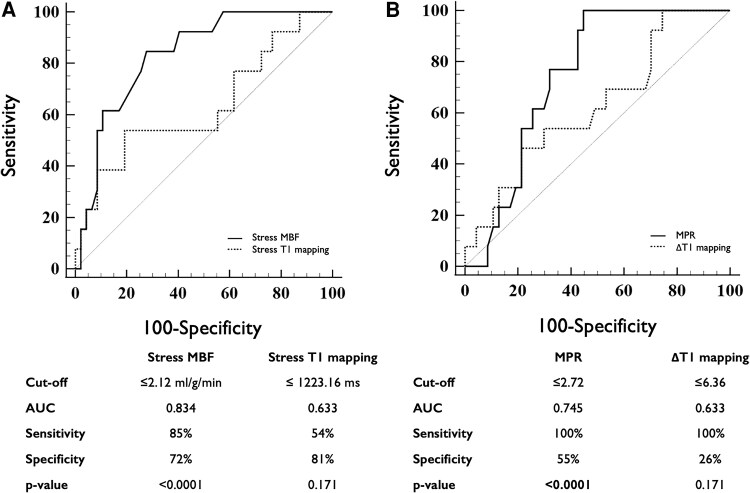
Methods and results: This study retrospectively analysed 51 patients with suspected obstructive CAD who underwent CMR including rest and adenosine stress first-pass perfusion and native T1 mapping (MOLLI). A moderate correlation was found between pooled rest and stress native T1 mapping and myocardial blood flow (Pearson's r = 0.476; P < 0.001). When stratified by myocardial perfusion reserve (MPR), ischaemic myocardium had significantly lower stress T1 mapping values (P < 0.001) and ΔT1 (P = 0.005) vs. nonischaemic myocardium. Male sex and history of diabetes were independently associated with lower ΔT1. The optimal cut-off value of ΔT1 to detect impaired MPR on a per-vessel basis was ≤5.4%, with an area under the curve of 0.662 (95% CI: 0.563-0.752, P = 0.003), sensitivity of 84% (95% CI: 67-95), and specificity of 46% (95% CI: 34-58). When validated against ICA, stress T1 and ΔT1 did not reach statistical significance in detecting obstructive CAD.
Conclusion: ΔT1 is significantly influenced by sex and comorbidities and has poor diagnostic accuracy for detecting myocardial ischaemia. Therefore, the clinical utility of ΔT1 in a real-world cohort of patients to detect obstructive CAD is limited.
Keywords: T1 mapping; cardiovascular magnetic resonance; coronary artery disease; myocardial ischaemia; quantitative perfusion.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures



Comment in
-
T1 mapping is not ready to replace the use of contrast agents in stress CMR.Eur Heart J Cardiovasc Imaging. 2025 May 30;26(6):991-992. doi: 10.1093/ehjci/jeaf098. Eur Heart J Cardiovasc Imaging. 2025. PMID: 40114389 No abstract available.
References
-
- Taylor AJ, Salerno M, Dharmakumar R, Jerosch-Herold M. T1 mapping: basic techniques and clinical applications. JACC Cardiovasc Imaging 2016;9:67–81. - PubMed
-
- Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017;19:75. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
