

Estimating the potential health and economic impacts of new tuberculosis vaccines under varying delivery strategies in Delhi and Gujarat, India: a modelling study
- PMID: 39957772
- PMCID: PMC11827003
- DOI: 10.1016/j.lansea.2024.100424
Estimating the potential health and economic impacts of new tuberculosis vaccines under varying delivery strategies in Delhi and Gujarat, India: a modelling study
Abstract
Background: India has the largest tuberculosis burden, but the all-age prevalence in 2021 ranged from 747/100,000 in Delhi to 137/100,000 in Gujarat. No modelling studies have compared the potential impact of new tuberculosis vaccines in regions with differing disease and infection prevalence.
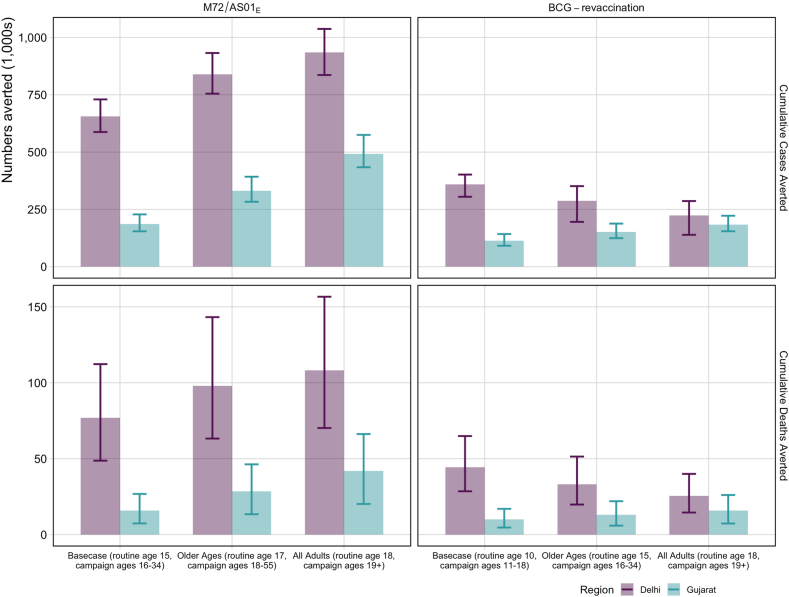
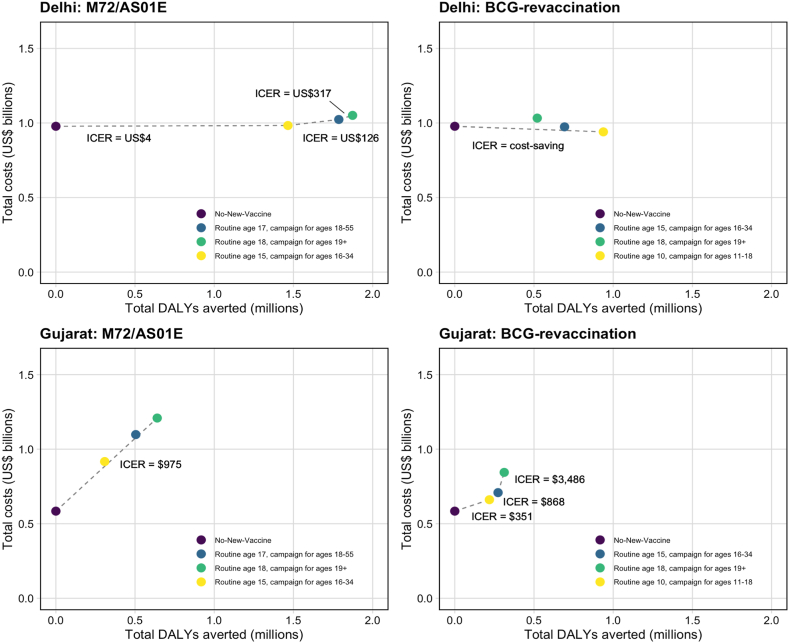
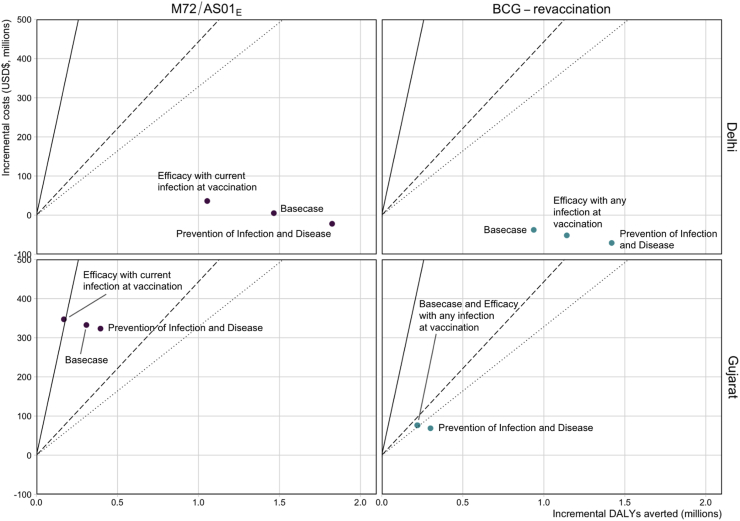
Methods: We used modelling to simulate hypothetical scenarios of introducing M72/AS01E (with 50% efficacy to prevent disease) and BCG-revaccination (with 45% efficacy to prevent infection) in Delhi and Gujarat.
Findings: The hypothetical M72/AS01E scenario could avert 16.0% of cases and 14.4% of deaths in Delhi, and 8.5% of cases and 7.6% of deaths in Gujarat between 2025 and 2050. The hypothetical BCG-revaccination scenario could avert 8.8% of cases and 8.3% of deaths in Delhi, and 5.1% of cases and 4.8% of deaths in Gujarat between 2025 and 2050.
Interpretation: Additional trials for both vaccines are underway, which will provide further evidence on the vaccine efficacy and narrow the range of uncertainty on the estimates.
Funding: Bill & Melinda Gates Foundation (INV-001754).
Keywords: Cost-effectiveness; Health economics; India; Mathematical modelling; Subnational; Tuberculosis; Vaccines.
© 2024 The Author(s).
Conflict of interest statement
RCH reports employment by Sanofi Pasteur, unrelated to tuberculosis and outside the submitted work. NAM received consulting fees from The Global Fund to Fight AIDS, Tuberculosis and Malaria, and WHO, and reports funding to their institution from the U.S. Centers for Disease Control and Prevention, the Bill & Melinda Gates Foundation, NIH, and U.S. Council of State and Territorial Epidemiologists. RGW is also funded for other work by the Wellcome Trust (218261/Z/19/Z), NIH (1R01AI147321-01), EDCTP (RIA208D-2505 B), UK MRC (CCF 17-7779 via SET Bloomsbury), ESRC (ES/P008011/1), BMGF (OPP1084276, OPP1135288 & INV-001754), and WHO. All other authors declare no conflicts of interest.
Figures
Update of
-
The potential health and economic impacts of new tuberculosis vaccines under varying delivery strategies in Delhi and Gujarat, India: a modelling study.medRxiv [Preprint]. 2023 Sep 27:2023.09.27.23296211. doi: 10.1101/2023.09.27.23296211. medRxiv. 2023. Update in: Lancet Reg Health Southeast Asia. 2024 May 16;31:100424. doi: 10.1016/j.lansea.2024.100424. PMID: 37808744 Free PMC article. Updated. Preprint.
References
-
- Indian Council of Medical Research (ICMR) 2022. National TB prevalence survey India 2019-2021.
-
- Ministry of Health and Family Welfare, Government of India . 2023. India TB report 2023.
-
- Tait D.R., Hatherill M., Van Der Meeren O., et al. Final analysis of a trial of M72/AS01E vaccine to prevent tuberculosis. N Engl J Med. 2019;381:2429–2439. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
