

Improved outcomes of endoscopic treatment for delayed perforation following endoscopic submucosal dissection for gastric epithelial neoplasms
- PMID: 39958656
- PMCID: PMC11827739
- DOI: 10.1055/a-2451-7835
Improved outcomes of endoscopic treatment for delayed perforation following endoscopic submucosal dissection for gastric epithelial neoplasms
Abstract
Background and study aims: Emergency surgery is usually required for patients with delayed perforation after gastric endoscopic submucosal dissection (ESD); however, cases of successful endoscopic treatment recently have been reported. Here, we elucidated the usefulness of endoscopic intervention for patients with delayed perforation.
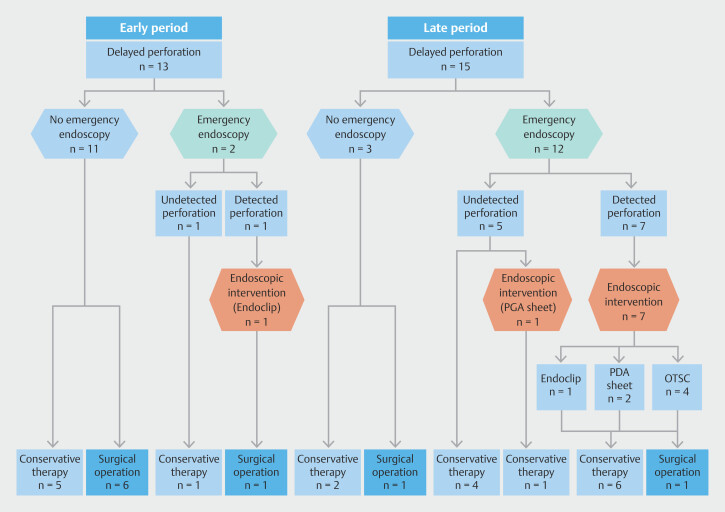
Patients and methods: Patients who underwent gastric ESD from 2005 to 2022 were assessed for eligibility. Delayed perforation was defined as no intraprocedural perforation after the ESD but subsequent development of peritoneal irritation and free air on computed tomography scan. Participants were divided into early- and late-period groups based on time (October 2015) of implementation of the polyglycolic acid (PGA) sheet and the over-the-scope clip (OTSC) in clinical practice. We evaluated changes in incidence of required surgery.
Results: Among the 5,048 patients who underwent gastric ESD, delayed perforation occurred in 28 patients (0.6%, 95% confidence interval [CI] 0.4%-0.8%). Incidence of delayed perforation did not differ significantly between the early- and late-period groups (0.5% vs. 0.6%). The proportion of patients who underwent surgery was significantly smaller in the late-period group than in the early-period group (54% vs. 13%, odds ratio [OR] 0.14, 95% CI 0.02-0.83; P = 0.042); this was confirmed by multivariate analysis (adjusted OR 0.04, 95% CI 0.002-0.9; P = 0.043) after adjustment for age, sex, Charlson's comorbidity index, tumor location, and size.
Conclusions: Endoscopic intervention using PGA sheets and OTSC was associated with a low incidence of required surgery for delayed perforation after gastric ESD and is recommended.
Keywords: Endoscopic resection (ESD, EMRc, ...); Endoscopy Upper GI Tract; Performance and complications; Precancerous conditions & cancerous lesions (dysplasia and cancer) stomach; Quality and logistical aspects.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflict of Interest Dr. Noriya Uedo is an Editorial Board member of EIO and a co-author of this article. To minimize bias, he was excluded from all editorial decision-making related to the acceptance of this article for publication. The other authors have no potential conflicts of interest to disclose.
Figures



References
LinkOut - more resources
Full Text Sources
Miscellaneous