

Combined inhibition of ribonucleotide reductase and WEE1 induces synergistic anticancer activity in Ewing's sarcoma cells
- PMID: 39962391
- PMCID: PMC11831844
- DOI: 10.1186/s12885-025-13691-2
Combined inhibition of ribonucleotide reductase and WEE1 induces synergistic anticancer activity in Ewing's sarcoma cells
Abstract
Background: Ewing's sarcoma is a childhood bone and soft tissue cancer with poor prognosis. Treatment outcomes for Ewing's sarcoma patients have improved only modestly over the past decades, making the development of new treatment strategies paramount. In this study, the combined targeting of ribonucleotide reductase (RNR) and WEE1 was explored for its effectiveness against Ewing's sarcoma cells.
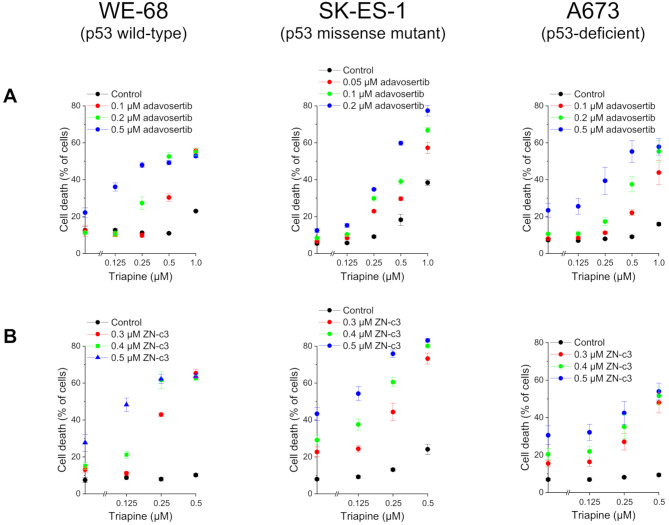
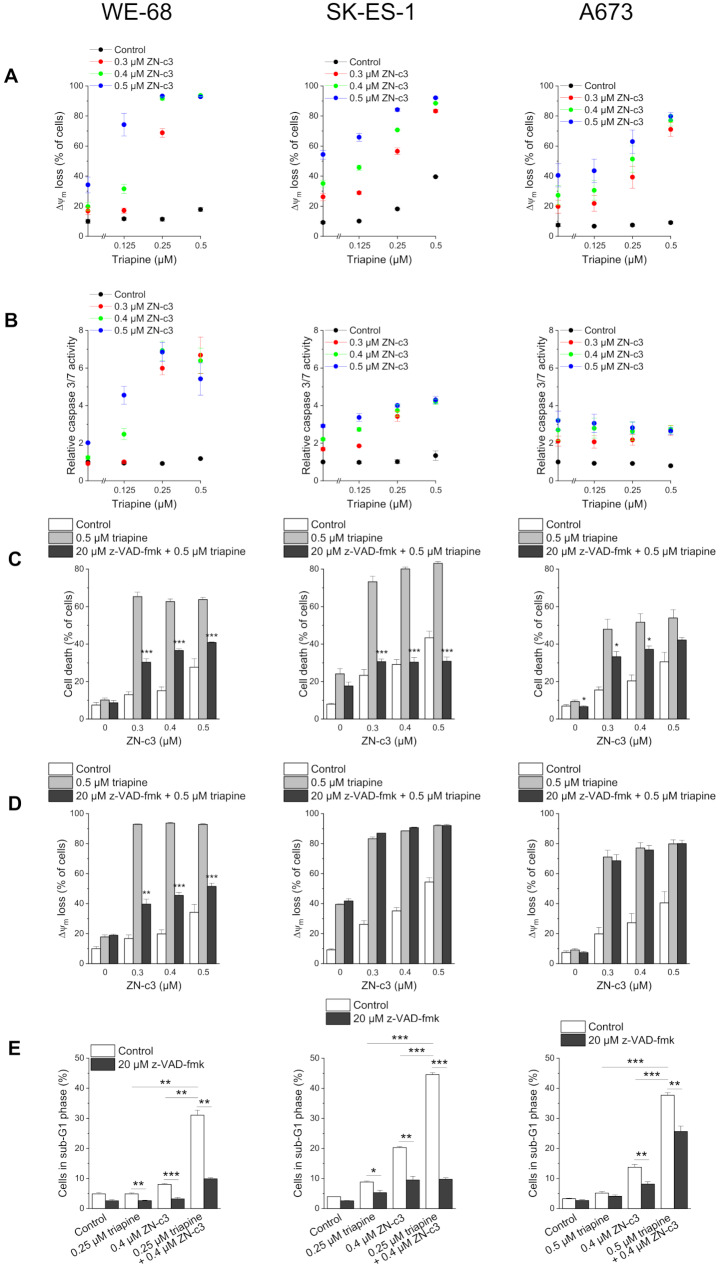
Methods: The RNR inhibitor triapine and the WEE1 inhibitors adavosertib and ZN-c3 were tested in p53 wild-type and p53 mutant Ewing's sarcoma cells. The combination of adavosertib with the PARP inhibitors olaparib and veliparib was tested for comparison. Combinatorial effects were determined by flow cytometric analyses of cell death, loss of mitochondrial membrane potential and DNA fragmentation as well as by caspase 3/7 activity assay, immunoblotting and real-time RT-PCR. The drug interactions were assessed using combination index analysis.
Results: RNR and WEE1 inhibitors were weakly to moderately effective on their own, but highly effective in combination. The combination treatments were similarly effective in p53 wild-type and p53 mutant cells. They synergistically induced cell death and cooperated to elicit mitochondrial membrane potential decay, to activate caspase 3/7 and to trigger DNA fragmentation, evidencing the induction of the apoptotic cell death cascade. They also cooperated to boost CHK1 phosphorylation, indicating augmented replication stress after combination treatment. In comparison, the combination of adavosertib with PARP inhibitors produced weaker synergistic effects.
Conclusion: Our findings show that combined inhibition of RNR and WEE1 was effective against Ewing's sarcoma in vitro. They thus provide a rationale for the evaluation of the potential of combined targeting of RNR and WEE1 in Ewing's sarcoma in vivo.
Keywords: Adavosertib; Ewing’s sarcoma; Olaparib; PARP; Ribonucleotide reductase; Targeted therapy; Triapine; Veliparib; WEE1; ZN-c3.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures




References
-
- Brennan B, Kirton L, Marec-Berard P, Gaspar N, Laurence V, Martin-Broto J, Sastre A, Gelderblom H, Owens C, Fenwick N, et al. Comparison of two chemotherapy regimens in patients with newly diagnosed Ewing sarcoma (EE2012): an open-label, randomised, phase 3 trial. Lancet. 2022;400(10362):1513–21. - DOI - PubMed
-
- Koch R, Gelderblom H, Haveman L, Brichard B, Jürgens H, Cyprova S, van den Berg H, Hassenpflug W, Raciborska A, Ek T, et al. High-dose treosulfan and melphalan as consolidation therapy versus standard therapy for high-risk (metastatic) ewing sarcoma. J Clin Oncol. 2022;40(21):2307–20. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
