

Impact of duration to endoscopy in patients with non-variceal upper gastrointestinal bleeding: propensity score matching analysis of real-world data from Thailand
- PMID: 39962393
- PMCID: PMC11834220
- DOI: 10.1186/s12876-025-03673-w
Impact of duration to endoscopy in patients with non-variceal upper gastrointestinal bleeding: propensity score matching analysis of real-world data from Thailand
Abstract
Background: The findings on mortality, rebleeding rate, and hospital stay in patients who underwent early vs. late endoscopy are conflicting. We aimed to compare in-hospital outcomes and medical resource use in patients with acute non-variceal upper gastrointestinal bleeding.
Methods: We retrospectively reviewed the medical records of patients with acute non-variceal upper gastrointestinal bleeding who underwent early or late endoscopy between 2016 and 2019. The primary outcome was in-hospital mortality. The secondary outcomes were the need for packed red blood cells and number of transfusions, the proportion of lesions with high-risk stigmata, endoscopic and additional hemostasis, in-hospital rebleeding, duration of stay, and admission cost. Statistical analysis was performed using Pearson's chi-squared or Fisher's exact test for categorical variables, Student's t-test, and Wilcoxon rank-sum test for continuous variables.
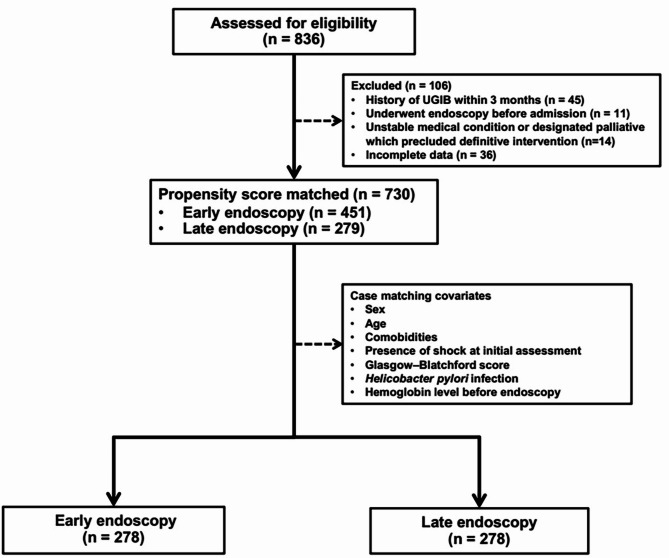
Results: Early and late endoscopies were performed on 451 and 279 patients, respectively. After 1:1 propensity score matching, 278 patients from each group were included, and patients' baseline characteristics were similar in the matched groups. Compared with the late group, the early group had a significantly increased rate of endoscopic hemostasis (22.7% vs. 13.7%, P = 0.006) and a low rate of packed red blood cell transfusion (53.6% vs. 61.9%, P = 0.048). Duration of stay and admission costs were significantly higher in the late group than in the early group (all P < 0.05). After adjusting for confounding factors, early endoscopy was positively associated with ulcers with high-risk stigmata (adjusted odds ratio = 1.83, P = 0.023) and endoscopic hemostasis (adjusted odds ratio = 1.97, P = 0.004). It was negatively associated with the need for packed red blood cell transfusion (adjusted odds ratio = 0.62, P = 0.017) and duration of stay (adjusted coefficient=-0.10, P < 0.001) with no impact on in-hospital mortality, rebleeding, or radiological interventions.
Conclusions: The timing of endoscopy does not affect in-hospital mortality or rebleeding rate. This study supports using early endoscopy in patients with acute non-variceal upper gastrointestinal bleeding based on the potential benefits and feasibility of medical resource use.
Keywords: Clinical outcomes; Early endoscopy; Medical resource use; Non-variceal upper gastrointestinal bleeding; Time to endoscopy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Institutional Review Board of Hatyai Hospital approved the study (protocol number: HYH EC 097-65-01). This study was conducted in accordance with the principles of the Declaration of Helsinki. Our Institutional Review Board deemed that no additional informed consent was required apart from the standard consent for endoscopy. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures

Similar articles
-
Optimal endoscopy timing in elderly patients presenting with acute non-variceal upper gastrointestinal bleeding.BMC Gastroenterol. 2024 Dec 2;24(1):444. doi: 10.1186/s12876-024-03541-z. BMC Gastroenterol. 2024. PMID: 39623308 Free PMC article.
-
Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline.Endoscopy. 2015 Oct;47(10):a1-46. doi: 10.1055/s-0034-1393172. Epub 2015 Sep 29. Endoscopy. 2015. PMID: 26417980
-
Outcome of non-variceal acute upper gastrointestinal bleeding in relation to the time of endoscopy and the experience of the endoscopist: a two-year survey.World J Gastroenterol. 2005 Dec 7;11(45):7122-30. doi: 10.3748/wjg.v11.i45.7122. World J Gastroenterol. 2005. PMID: 16437658 Free PMC article.
-
AGA Clinical Practice Update on Endoscopic Therapies for Non-Variceal Upper Gastrointestinal Bleeding: Expert Review.Gastroenterology. 2020 Sep;159(3):1120-1128. doi: 10.1053/j.gastro.2020.05.095. Epub 2020 Jun 20. Gastroenterology. 2020. PMID: 32574620 Review.
-
Acute, nonvariceal upper gastrointestinal bleeding.Curr Opin Crit Care. 2015 Apr;21(2):154-62. doi: 10.1097/MCC.0000000000000185. Curr Opin Crit Care. 2015. PMID: 25692808 Review.
Cited by
-
Clinical Impact of Red Blood Cell Transfusion Location on Gastrointestinal Bleeding Outcomes: Emergency Department vs. Inpatient Unit.Healthcare (Basel). 2025 Jul 9;13(14):1656. doi: 10.3390/healthcare13141656. Healthcare (Basel). 2025. PMID: 40724681 Free PMC article.
References
-
- Gralnek IM, Dumonceau JM, Kuipers EJ, Lanas A, Sanders DS, Kurien M, et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47:a1–46. - PubMed
-
- Colle I, Wilmer A, Le Moine O, Debruyne R, Delwaide J, Dhondt E, et al. Upper gastrointestinal tract bleeding management: Belgian guidelines for adults and children. Acta Gastroenterol Belg. 2011;74:45–66. - PubMed
-
- Rosenstock SJ, Møller MH, Larsson H, Johnsen SP, Madsen AH, Bendix J, et al. Improving quality of care in peptic ulcer bleeding: nationwide cohort study of 13,498 consecutive patients in the Danish clinical Register of emergency surgery. Am J Gastroenterol. 2013;108:1449–57. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
