

Second 'pop-off' of fetal giant urinoma: case report and review
- PMID: 39962415
- PMCID: PMC11834222
- DOI: 10.1186/s12884-025-07279-8
Second 'pop-off' of fetal giant urinoma: case report and review
Abstract
Background: Renal fornices rupture with urinoma formation in fetuses is an unusual condition that acts as a 'pop off' mechanism to buffer renal pelvis pressure. Ureteropelvic junction obstruction (UPJO) is the most common cause of prenatal hydronephrosis, but it rarely leads to the formation of urinoma. Fetal urinoma could be indicative of poor renal function after birth. We report a rare case of UPJO-related urinoma accompanied with urinary ascites, which ruptured during vaginal delivery.
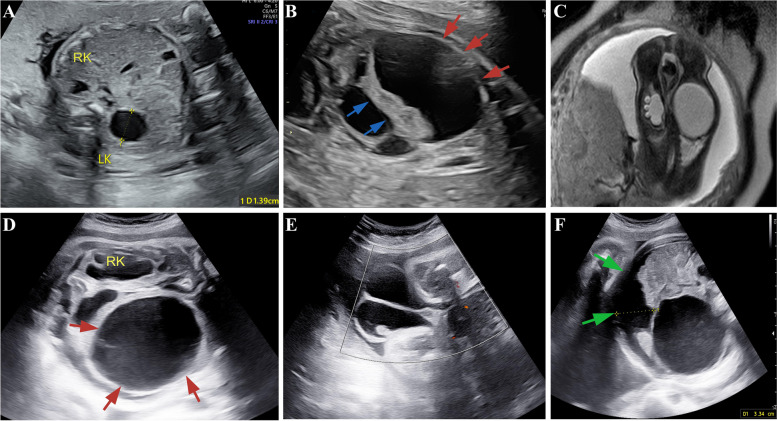
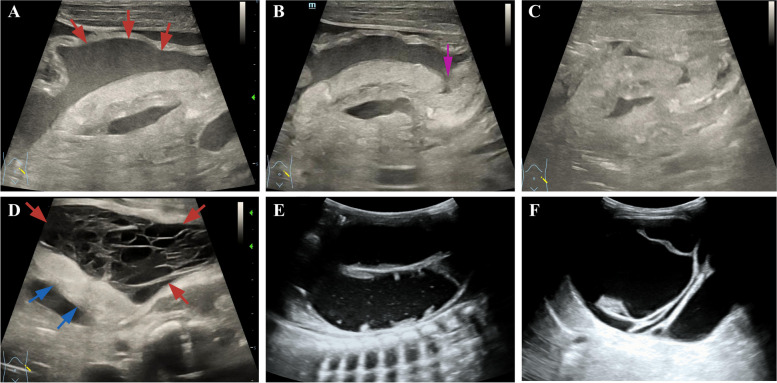
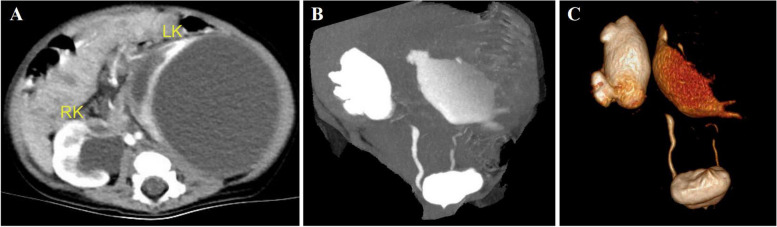
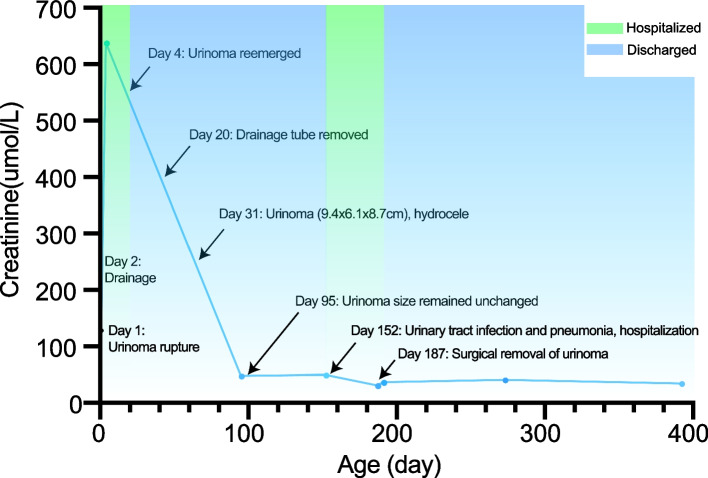
Case presentation: A 30-year-old woman was admitted to our hospital at 25+3 weeks gestation for fetal bilateral hydronephrosis. This probable case of UPJO became further complicated at 29+5 weeks with the presence of a urinoma around the left kidney and ascites. Afterwards, the urinoma gradually enlarged and the ascites worsened, accompanied by testicular hydrocele, pleural effusion, and polyhydramnios. The last prenatal ultrasound at 36+1 weeks disclosed that the size of the urinoma was approximately 9.0 × 6.3x8.7 cm. The amniotic membrane ruptured prematurely and a male infant was vaginally delivered at 37 weeks. The baby developed gradually worsening abdominal distension. Bedside US revealed the urinoma became irregular and smaller, accompanied by a significant increase in ascites. It was speculated that the urinoma might experience a secondary rupture. Ascites drainage was performed and the urinoma disappeared. But it reemerged 2 days later with a significant increase in serum creatinine. The parents opted to abandon treatment. Surprisingly, the infant developed good feeding and mental health after discharge. Serum creatinine returned to normal at 3 months. Due to compression of surrounding tissues by the huge urinoma, the infant accepted urinoma resection surgery at 6 months. By the age of one, the infant was developing normally without signs of renal impairment.
Conclusions: Prenatal identification of a large urinoma with urinary ascites requires necessary attention and appropriate management strategies. Prenatal urinoma drainage is indicated for large urinoma risking dystocia or rupture during delivery. Postnatal ascites requires active drainage to prevent creatinine and urea reabsorption and other complications. Small asymptomatic urinoma can be managed conservatively, but early surgery is recommended for large or recurrent urinoma exerting pressure on surrounding tissues.
Keywords: Case report; Prenatal diagnosis; Renal fornices rupture; Ultrasonography; Urinoma.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Ethics Committee of West China Second Hospital, Sichuan University. Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal. Competing interests: The authors declare no competing interests.
Figures
References
-
- Adorisio O, Silveri M, Colajacomo M, Bassani F, Rivosecchi M. The impact of perinatal urinoma formation on renal function: our experience and review of the literature. J Paediatr Child Health. 2011;47(4):217–22. 10.1111/j.1440-1754.2010.01927.x. - PubMed
-
- Lundar L, Aksnes G, Mørkrid L, Emblem R. Prenatal extravasation of urine seems to preserve renal function in boys with posterior urethral valves. J Pediatric urol. 2019;15(3):241.e1-.e7.10.1016/j.jpurol.2019.02.010 - PubMed
-
- Gorincour G, Rypens F, Toiviainen-Salo S, Grignon A, Lambert R, Audibert F, et al. Fetal urinoma: two new cases and a review of the literature. Ultrasound Obstet Gynecol. 2006;28(6):848–52. 10.1002/uog.2830. - PubMed
-
- Simonini C, Strizek B, Strömer A, Gembruch U, Geipel A. Prenatal diagnosis and outcome of fetal urinomas in relation to the underlying etiology. Prenatal Diagnosis. 2023;44:139–47. 10.1002/pd.6355. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
