

Oral Squamous Cell Carcinoma in Atrophic-Erosive Lichen Planus: 10-Year Rehabilitative Case Report
- PMID: 39963098
- PMCID: PMC11832267
- DOI: 10.1155/crid/5548590
Oral Squamous Cell Carcinoma in Atrophic-Erosive Lichen Planus: 10-Year Rehabilitative Case Report
Abstract
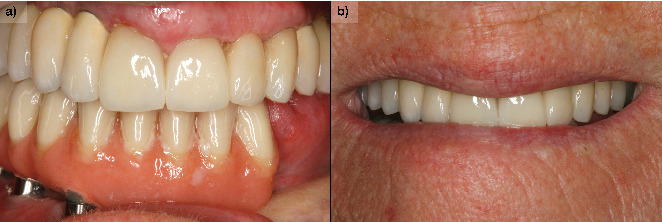
Patients with oral lichen planus can sometimes develop malignancy of the process and develop oral squamous cell carcinoma or another type of cancer. Close monitoring of the lesions and early diagnosis is important to increase patient survival. Once cancer treatment has been performed, the therapeutic options for restoring masticatory and phonatory function, in addition to resolving the aesthetic sequelae, are important. In the present clinical case, we show a patient who was treated and followed over a long period of time for both her carcinoma and her subsequent rehabilitation with implants.
Copyright © 2025 Eduardo Anitua et al. Case Reports in Dentistry published by John Wiley & Sons Ltd.
Conflict of interest statement
E.A. is the scientific director of BTI Biotechnology Institute, the company that has developed the Endoret PRGF technology and commercializes BTI implant system. L.P. has no conflict of interest. M.H.A. is a researcher at BTI Biotechnology Institute I MAS D.
Figures










References
Publication types
LinkOut - more resources
Full Text Sources
