

Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) Impacts Long-Term Outcomes After Curative-Intent Surgery for Hepatocellular Carcinoma
- PMID: 39964081
- PMCID: PMC11950813
- DOI: 10.1111/apt.70002
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) Impacts Long-Term Outcomes After Curative-Intent Surgery for Hepatocellular Carcinoma
Abstract
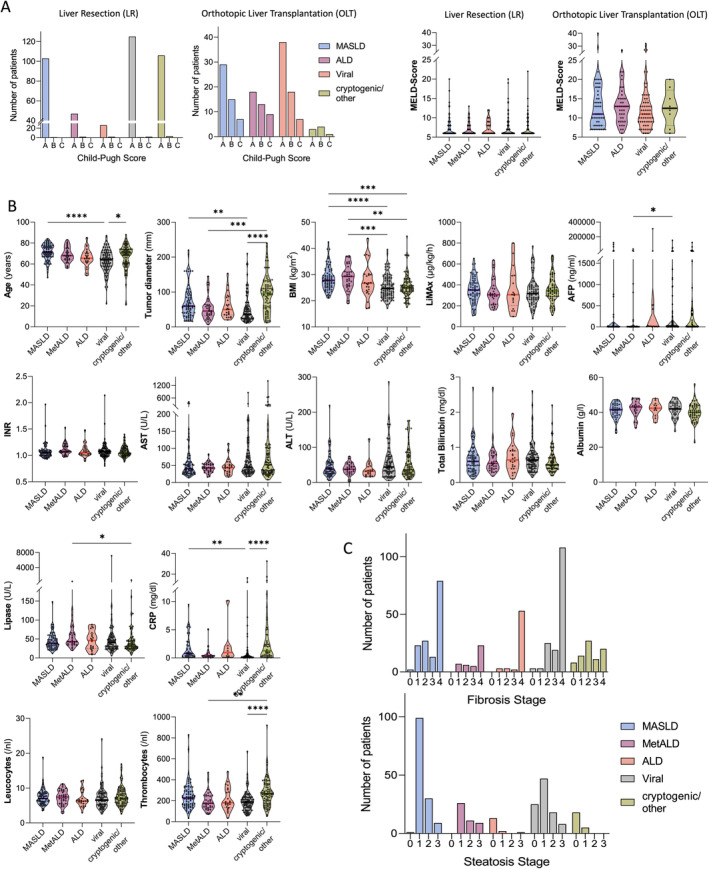
Background: Curative surgery for hepatocellular carcinoma (HCC) includes liver resection (LR) and orthotopic liver transplantation (OLT). Due to the obesity epidemic, metabolic dysfunction-associated steatotic liver disease (MASLD) is a frequent HCC aetiology that often coincides with increased alcohol consumption, termed MetALD, or even alcohol-associated liver disease (ALD).
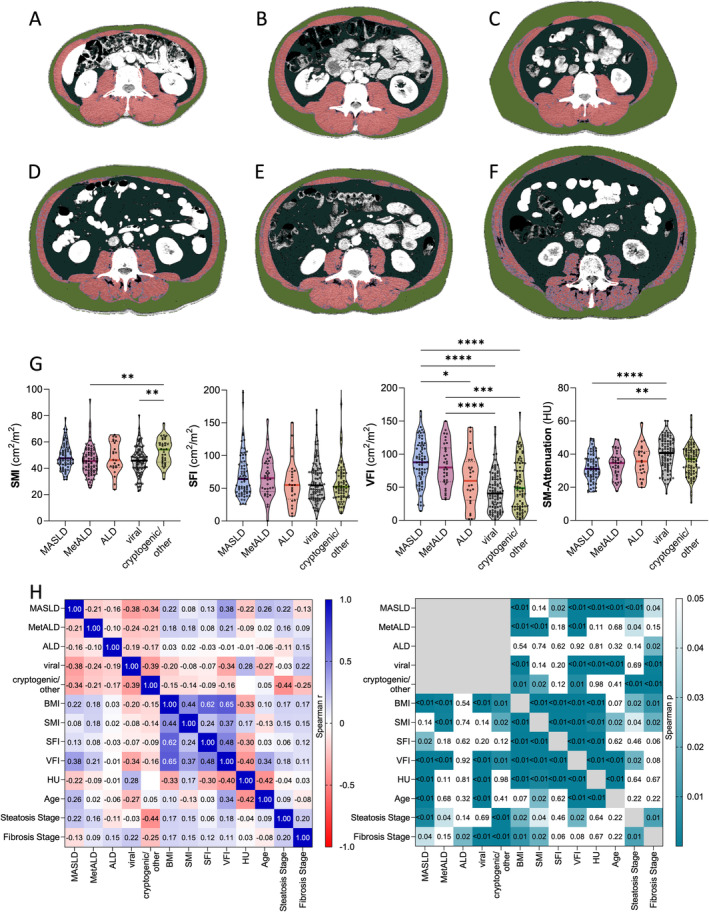
Methods: Patients undergoing LR or OLT for HCC at Charité-Universitätsmedizin Berlin (2010-2020) were included in this retrospective cohort study investigating disease aetiology, time to recurrence (TTR), overall survival (OS) and CT-based body composition.
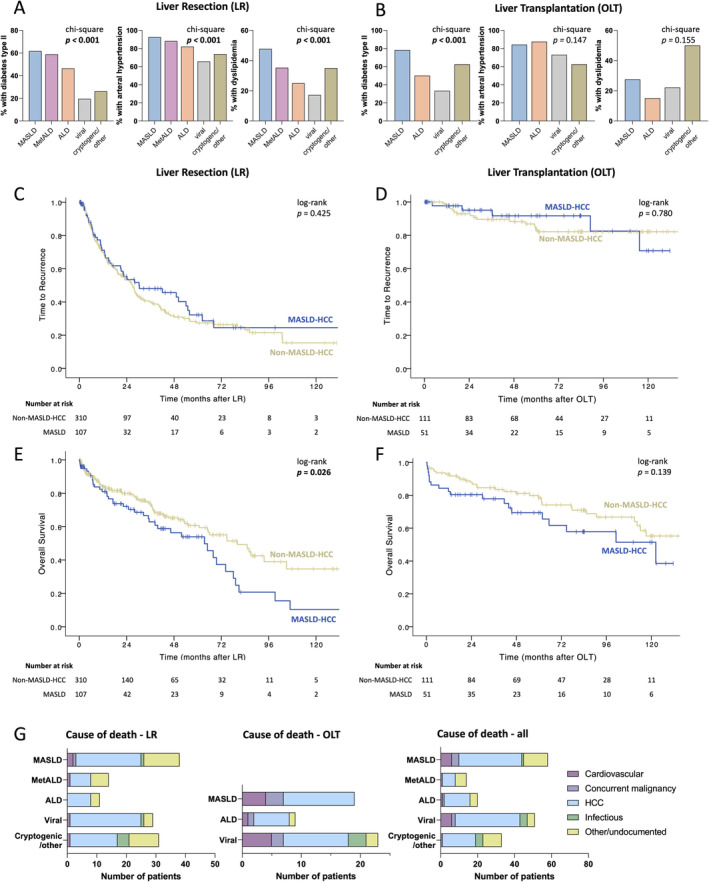
Results: Out of 579 patients with HCC, 417 underwent LR and 162 OLT. Tumour aetiologies were viral n = 191 (33.0%), MASLD n = 158 (27.3%), MetALD n = 51 (8.8%), ALD n = 68 (11.7%) and other/cryptogenic n = 111 (19.2%). Patients with MASLD and MetALD had more intramuscular (p < 0.001, p = 0.015) and visceral fat (both p < 0.001) than patients with non-metabolic dysfunction aetiologies. Patients with MASLD-HCC had comparable TTR (median 26 months, [95% CI: 23-31] vs. 30 months [95% CI: 4-57], p = 0.425) but shorter OS than patients with other HCC aetiologies (63 months [95% CI: 42-84] vs. 80 months [95% CI: 60-100], hazard ratio: 1.53 [95% CI: 1.050-2.229], p = 0.026) after LR. Multivariate analysis confirmed MASLD aetiology, portal vein thrombosis and MELD score ≥ 10 as independent prognostic factors for OS in LR (adjusted p = 0.021,p < 0.001,p = 0.003), even after excluding in-hospital mortality (adjusted p = 0.016,p = 0.002,p = 0.002). Causes of death were similar in MASLD and non-MASLD aetiology.
Conclusions: Patients with HCC undergoing LR and meeting the new MASLD criteria have significantly shorter OS. This study provides empirical prognostic evidence for the novel MASLD/MetALD classification in a large European cohort of patients undergoing curative-intent HCC therapy.
© 2025 The Author(s). Alimentary Pharmacology & Therapeutics published by John Wiley & Sons Ltd.
Conflict of interest statement
G.L. reports receiving research funding and speakers' fees from Astellas Pharma, XVIVO, Bridge to Life, Organ recovery systems, Wyss Liver4Life, Orphalan and Aferetica S.R.L., and is on the advisory board of OrganOx, outside the submitted work. C.E. reports receiving an Else Kröner Fresenius Excellence Scholarship (German Research Foundation, DFG) and an EU‐Horizon grant, has shares with UCL Spin‐off company Hepyx Ltd., has received consulting fees from and is on the advisory board of Albireo/Ipsen and Boehringer Ingelheim, lecture honoraria/ travel support from Gilead and Albireo/Ipsen. F.T. reports research funding to his institution from AstraZeneca, MSD, Gilead, Agomab, consulting fees from AstraZeneca, Gilead, GSK, Abbvie, Alnylam, BMS, Intercept, Inventiva, Pfizer, Novartis, Novo Nordisk, MSD, Sanofi, lecture honoraria/travel support from Gilead, AbbVie, Falk, Merz, Intercept, Sanofi, Astra Zeneca, Orphalan, and is on the advisory board of Sanofi and Pfizer. The remaining authors have no conflicts of interest to declare.
Figures

Similar articles
-
Metabolic Dysfunction-Associated Steatotic Liver Disease and All-Cause and Cause-Specific Mortality.Diabetes Metab J. 2025 Jan;49(1):80-91. doi: 10.4093/dmj.2024.0042. Epub 2024 Aug 28. Diabetes Metab J. 2025. PMID: 39197834 Free PMC article.
-
Liver Cancer Risk Across Metabolic Dysfunction-Associated Steatotic Liver Disease and/or Alcohol: A Nationwide Study.Am J Gastroenterol. 2025 Feb 1;120(2):410-419. doi: 10.14309/ajg.0000000000002920. Epub 2024 Jun 27. Am J Gastroenterol. 2025. PMID: 38934496
-
Liver transplant for hepatocellular carcinoma in metabolic dysfunction-associated steatotic liver disease versus other etiologies: A meta-analysis.Dig Liver Dis. 2025 Feb;57(2):362-369. doi: 10.1016/j.dld.2024.09.025. Epub 2024 Oct 29. Dig Liver Dis. 2025. PMID: 39472175
-
Modifiable Risk Factors for Hepatocellular Carcinoma in Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease: A Meta-Analysis.Am J Med. 2024 Nov;137(11):1072-1081.e32. doi: 10.1016/j.amjmed.2024.06.031. Epub 2024 Jul 22. Am J Med. 2024. PMID: 39047929
-
Impact of Metabolic Dysfunction-Associated Fatty/Steatotic Liver Disease on Hepatocellular Carcinoma Incidence and Long-Term Prognosis Post-Liver Resection: A Systematic Review and Meta-Analysis.Acad Radiol. 2025 Jan 21:S1076-6332(25)00003-0. doi: 10.1016/j.acra.2025.01.003. Online ahead of print. Acad Radiol. 2025. PMID: 39843280 Review.
References
-
- El‐Serag H. B., Siegel A. B., Davila J. A., et al., “Treatment and Outcomes of Treating of Hepatocellular Carcinoma Among Medicare Recipients in the United States: A Population‐Based Study,” Journal of Hepatology 44, no. 1 (2006): 158–166. - PubMed
-
- Liver EAftSot , “EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma,” Journal of Hepatology 69, no. 1 (2018): 182–236. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous