

SEX DIFFERENCES IN SEPSIS-RELATED ACUTE RESPIRATORY DISTRESS SYNDROME AND OTHER SHORT-TERM OUTCOMES AMONG CRITICALLY ILL PATIENTS WITH SEPSIS: A RETROSPECTIVE STUDY IN CHINA
- PMID: 39965585
- PMCID: PMC12039918
- DOI: 10.1097/SHK.0000000000002555
SEX DIFFERENCES IN SEPSIS-RELATED ACUTE RESPIRATORY DISTRESS SYNDROME AND OTHER SHORT-TERM OUTCOMES AMONG CRITICALLY ILL PATIENTS WITH SEPSIS: A RETROSPECTIVE STUDY IN CHINA
Abstract
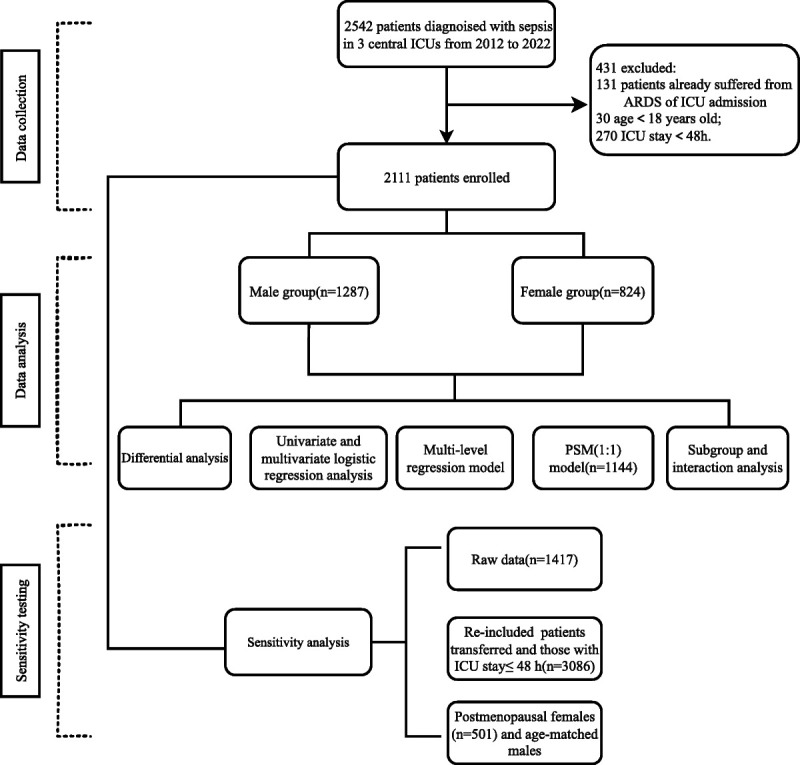
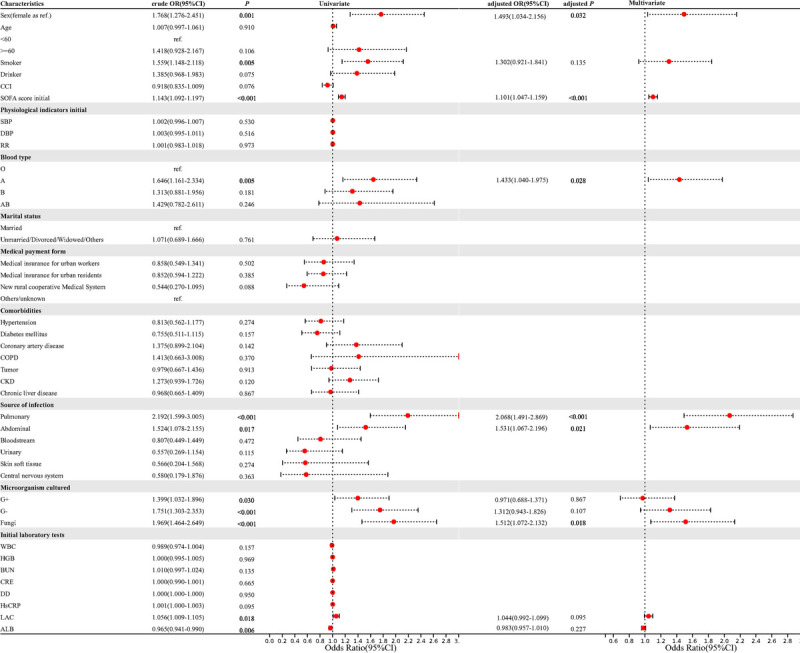
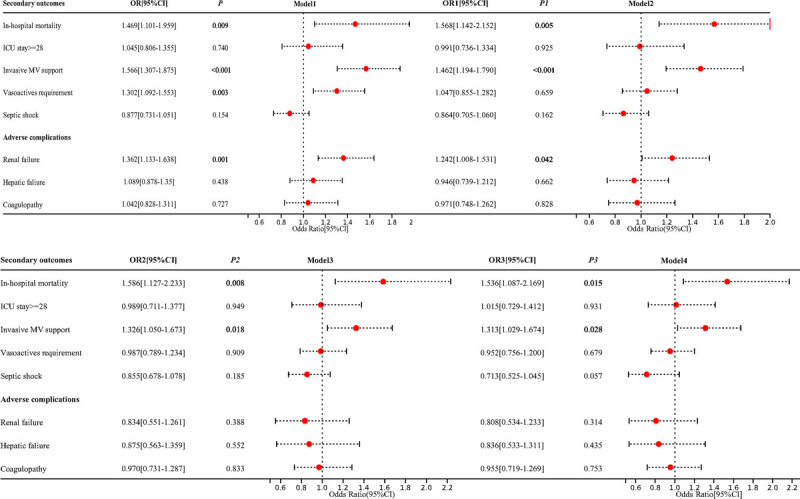
Background: The evidence of sex disparity in acute respiratory distress syndrome (ARDS) is scarce and varies widely. Objective: This observational, retrospective study aimed to determine the effect of sex on the sepsis-related ARDS and other short outcomes in critically ill patients with sepsis. Methods: A total of 2,111 adult patients with sepsis who were admitted to three central intensive care units (ICUs) of Wuhan Tongji Hospital between 2012 and 2022 were included in our analysis. Sex was considered as an exposure factor, with sepsis-related ARDS as the primary outcome, and in-hospital mortality, invasive mechanical ventilation support, septic shock, and other complications as secondary outcomes. Results: Among the 2,111 enrolled patients, 1,287 were males (61%) and 824 were females (39%). The incidence of sepsis-related ARDS was higher in males compared to females ( P = 0.001), as well as in-hospital mortality ( P = 0.009). Multivariate logistic analysis demonstrated that male sex remained independently associated with an increased risk of sepsis-related ARDS (adjusted odds ratio [aOR] = 1. 493 [1.034-2.156], P = 0.032). Propensity score matching analysis also indicated that males had 58% higher odds of developing sepsis-related ARDS (aOR = 1.584 [1.022-2.456], P = 0.040). Regarding secondary outcomes, male sex was identified as a risk factor for in-hospital mortality (aOR = 1.536 [1.087-2.169], P = 0.015) and invasive mechanical ventilation support (aOR = 1.313 [1.029-1.674], P = 0.028) in the fully adjusted model. Sensitivity analysis that included postmenopausal females and age-matched male counterparts showed that male sex still remained to be a risk factor of developing sepsis-related ARDS (aOR = 1.968 [1.241-3.120], P = 0.004). Conclusions: Male sex was identified as an independent risk factor for sepsis-related ARDS and in-hospital mortality among critically ill patients with sepsis. Given the retrospective design of this study, the relationship between sex and sepsis-related ARDS requires further validation through large-scale randomized controlled trials in the future.
Keywords: Sex difference; critical care; male; mortality; sepsis-related acute respiratory distress syndrome.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Shock Society.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
The epidemiology of acute respiratory distress syndrome in patients presenting to the emergency department with severe sepsis.Shock. 2013 Nov;40(5):375-81. doi: 10.1097/SHK.0b013e3182a64682. Shock. 2013. PMID: 23903852 Free PMC article.
-
Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study.Lancet Respir Med. 2020 May;8(5):475-481. doi: 10.1016/S2213-2600(20)30079-5. Epub 2020 Feb 24. Lancet Respir Med. 2020. PMID: 32105632 Free PMC article.
-
The impact of cardiac dysfunction on acute respiratory distress syndrome and mortality in mechanically ventilated patients with severe sepsis and septic shock: an observational study.J Crit Care. 2015 Feb;30(1):65-70. doi: 10.1016/j.jcrc.2014.07.027. Epub 2014 Aug 7. J Crit Care. 2015. PMID: 25179413 Free PMC article.
-
Corticosteroids in the prevention and treatment of acute respiratory distress syndrome (ARDS) in adults: meta-analysis.BMJ. 2008 May 3;336(7651):1006-9. doi: 10.1136/bmj.39537.939039.BE. Epub 2008 Apr 23. BMJ. 2008. PMID: 18434379 Free PMC article. Review.
-
Immunonutrition for acute respiratory distress syndrome (ARDS) in adults.Cochrane Database Syst Rev. 2019 Jan 24;1(1):CD012041. doi: 10.1002/14651858.CD012041.pub2. Cochrane Database Syst Rev. 2019. PMID: 30677127 Free PMC article.
References
-
- Bellani G Laffey JG Pham T, et al. . Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
