

Breast cancer: pathogenesis and treatments
- PMID: 39966355
- PMCID: PMC11836418
- DOI: 10.1038/s41392-024-02108-4
Breast cancer: pathogenesis and treatments
Abstract
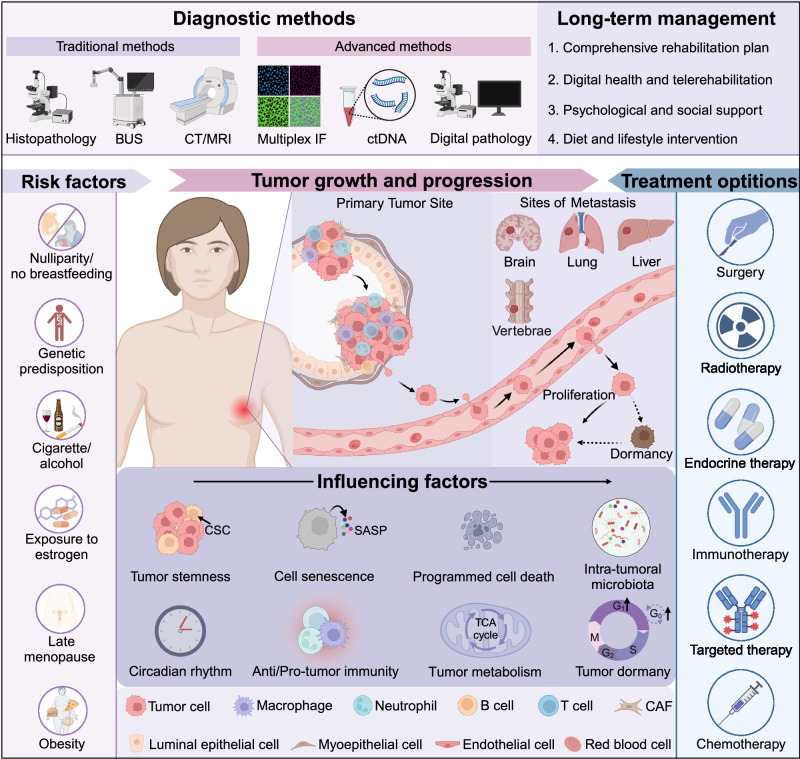
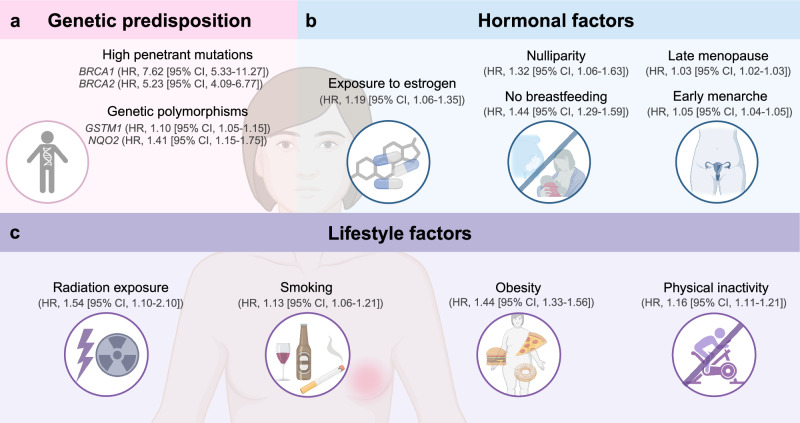
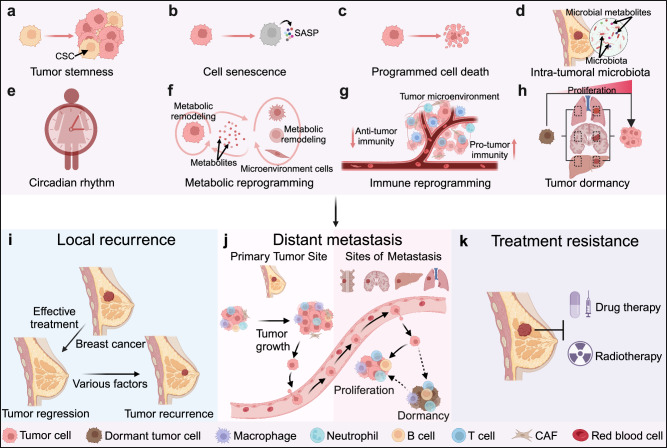
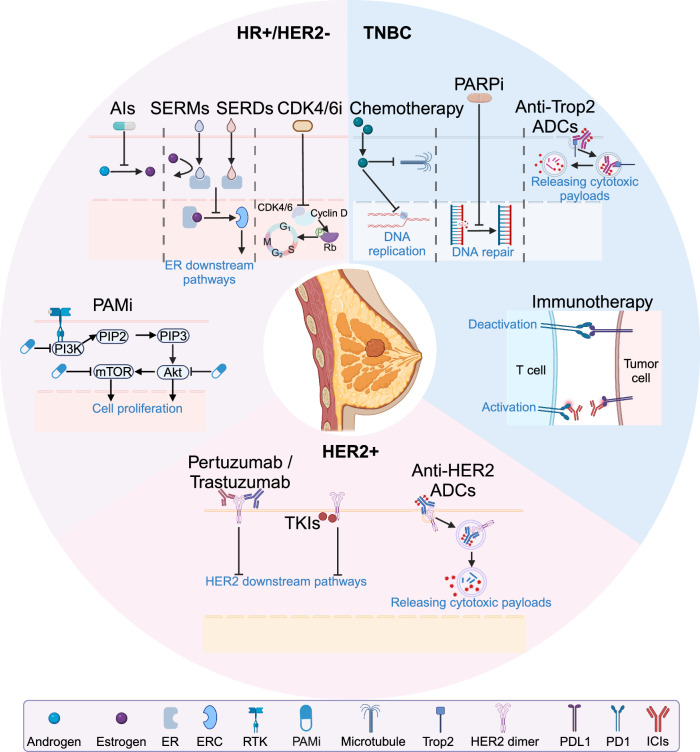
Breast cancer, characterized by unique epidemiological patterns and significant heterogeneity, remains one of the leading causes of malignancy-related deaths in women. The increasingly nuanced molecular subtypes of breast cancer have enhanced the comprehension and precision treatment of this disease. The mechanisms of tumorigenesis and progression of breast cancer have been central to scientific research, with investigations spanning various perspectives such as tumor stemness, intra-tumoral microbiota, and circadian rhythms. Technological advancements, particularly those integrated with artificial intelligence, have significantly improved the accuracy of breast cancer detection and diagnosis. The emergence of novel therapeutic concepts and drugs represents a paradigm shift towards personalized medicine. Evidence suggests that optimal diagnosis and treatment models tailored to individual patient risk and expected subtypes are crucial, supporting the era of precision oncology for breast cancer. Despite the rapid advancements in oncology and the increasing emphasis on the clinical precision treatment of breast cancer, a comprehensive update and summary of the panoramic knowledge related to this disease are needed. In this review, we provide a thorough overview of the global status of breast cancer, including its epidemiology, risk factors, pathophysiology, and molecular subtyping. Additionally, we elaborate on the latest research into mechanisms contributing to breast cancer progression, emerging treatment strategies, and long-term patient management. This review offers valuable insights into the latest advancements in Breast Cancer Research, thereby facilitating future progress in both basic research and clinical application.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures


References
-
- Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.74, 229–263 (2024). - PubMed
-
- Giaquinto, A. N. et al. Breast cancer statistics, 2022. CA Cancer J. Clin.72, 524–541 (2022). - PubMed
-
- Loibl, S., Poortmans, P., Morrow, M., Denkert, C. & Curigliano, G. Breast cancer. Lancet397, 1750–1769 (2021). - PubMed
-
- Siegel, R. L., Giaquinto, A. N. & Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin.74, 12–49 (2024). - PubMed
-
- Hickey, M. et al. Managing menopause after cancer. Lancet403, 984–996 (2024). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
