

Identification of digital twins to guide interpretable AI for diagnosis and prognosis in heart failure
- PMID: 39966509
- PMCID: PMC11836287
- DOI: 10.1038/s41746-025-01501-9
Identification of digital twins to guide interpretable AI for diagnosis and prognosis in heart failure
Abstract
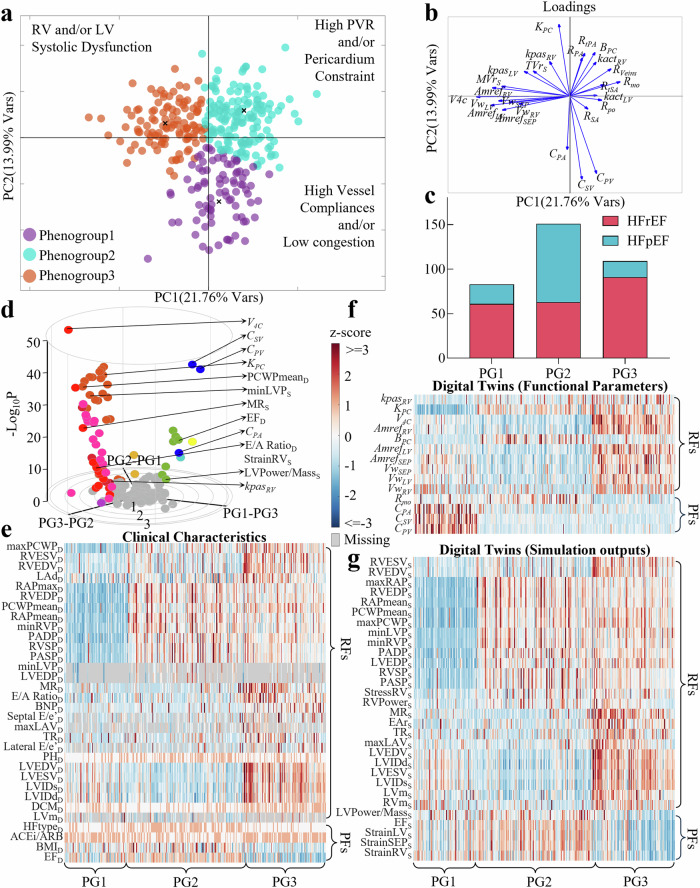
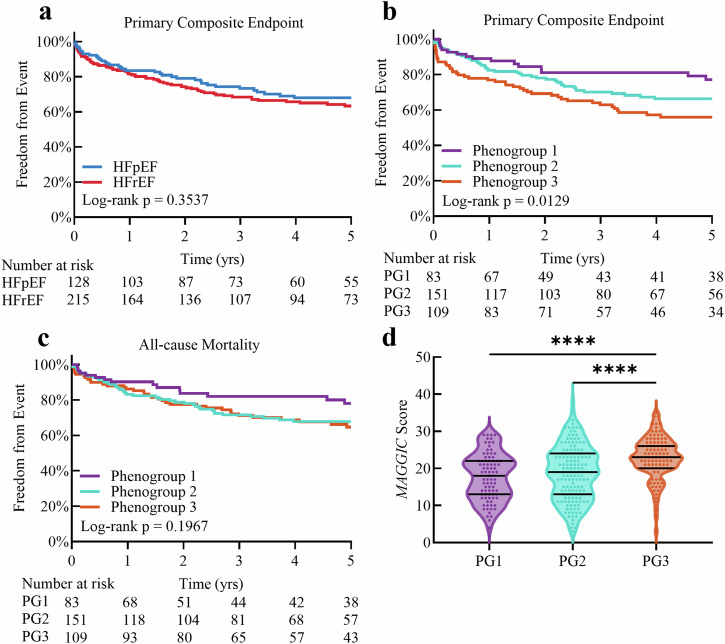
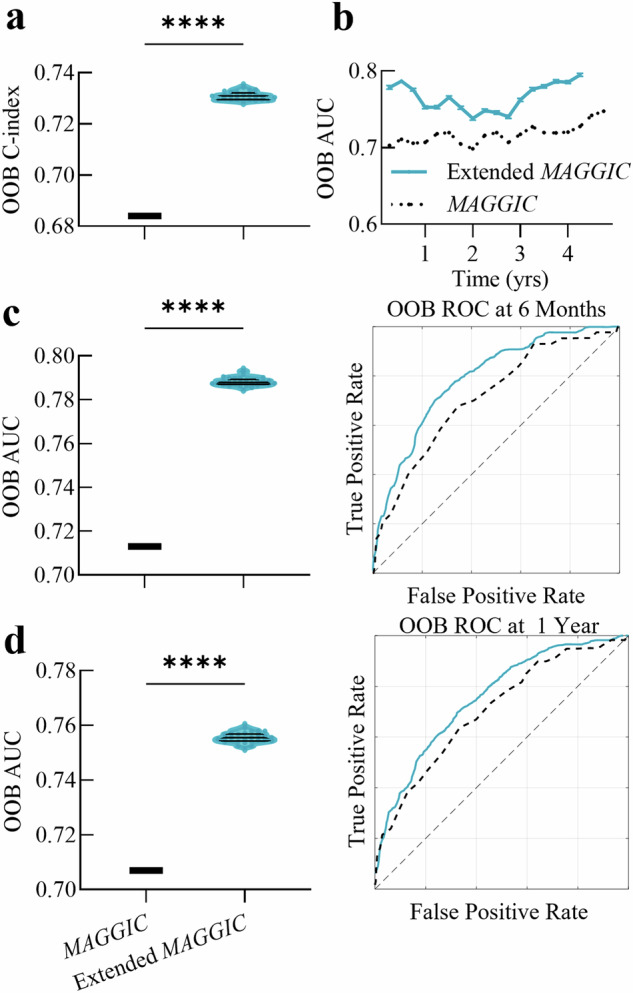
Heart failure (HF) is a highly heterogeneous condition, and current methods struggle to synthesize extensive clinical data for personalized care. Using data from 343 HF patients, we developed mechanistic computational models of the cardiovascular system to create digital twins. These twins, consisting of optimized measurable and unmeasurable parameters alongside simulations of cardiovascular function, provided comprehensive representations of individual disease states. Unsupervised machine learning applied to digital twin-derived features identified interpretable phenogroups and mechanistic drivers of cardiovascular death risk. Incorporating these features into prognostic AI models improved performance, transferability, and interpretability compared to models using only clinical variables. This framework demonstrates potential to enhance prognosis and guide therapy, paving the way for more precise, individualized HF management.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures





References
-
- McDonagh, T. A. et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J.42, 3599–3726 (2021). - PubMed
-
- Martin, S. S. et al. 2024 heart disease and stroke statistics: A report of us and global data from the american heart association. Circulation149, e347–e913 (2024). - PubMed
-
- Palau, P. et al. Effect of β-blocker withdrawal on functional capacity in heart failure and preserved ejection fraction. J. Am. Coll. Cardiol.78, 2042–2056 (2021). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
