

C3 glomerulopathy associated with mycoplasma pneumoniae infection and positive IgA staining
- PMID: 39966764
- PMCID: PMC11837633
- DOI: 10.1186/s12882-025-04010-9
C3 glomerulopathy associated with mycoplasma pneumoniae infection and positive IgA staining
Abstract
Background: Patients with C3 glomerulopathy (C3G) often have a history of infection, which implies that infection may lead to abnormal activation of the complement alternative pathway (CAP) and induce the development of C3G. However, patients with postinfectious glomerulonephritis (PIGN) often have a low serum C3 concentration and positive glomerular C3 staining, consistent with the activation of the CAP. PIGN, especially if it involves simultaneous IgA deposition, is often difficult to differentiate from C3G.
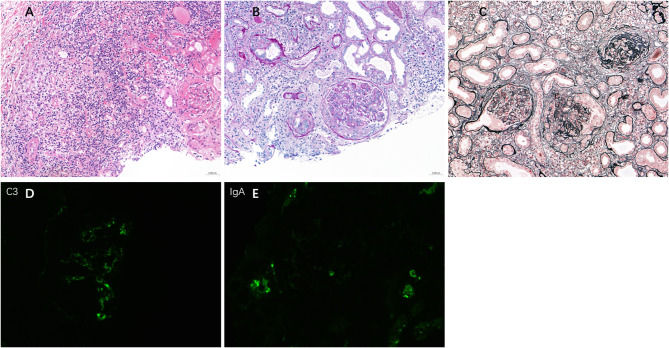
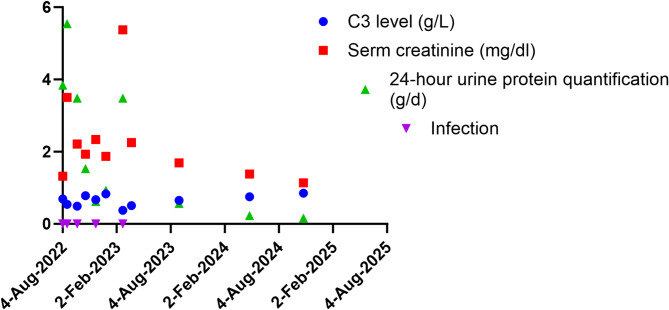
Case presentation: In this study, we report the consequences of Mycoplasma pneumoniae (MP) infection in a 66-year-old male Chinese patient, who developed persistent hypocomplementemia, gross hematuria, and rapidly progressive glomerulonephritis. The findings of the histologic examination of an initial renal biopsy were consistent with a diagnosis of IgA-dominant postinfectious glomerulonephritis. The sample was negative for Gd-IgA1 staining. After treatment with antibiotics, glucocorticoids, and mycophenolate mofetil, the patient's serum creatinine decreased from a peak of 387 µmol/L to 195 µmol/L prior to discharge, and there was a partial response in his urinary protein concentration. After 2 months, his serum C3 concentration had returned to normal. However, owing to reinfection with MP the patient's serum creatinine rapidly increased again to 475.07 µmol/L, and this was accompanied by a decrease in serum C3 concentration (> 8 months) and positivity for C3 nephritis factor. Examination of both renal biopsies showed stronger immunostaining for C3 than for IgA in the glomeruli.
Conclusion: Thus, MP infection can cause sustained activation of the CAP, leading to C3G. For patients with MP infection, if there is an ongoing decrease in complement C3 levels and a progressive increase in serum creatinine, it is crucial to be vigilant for possible C3G and to consider the use of immunosuppressive therapy in conjunction with anti-infective treatment to prevent the ongoing activation of the CAP.
Keywords: Mycoplasma pneumoniae; Acute kidney injury; C3 glomerulopathy; IgA-dominant postinfectious glomerulonephritis; Renal biopsy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Written informed consent to participate obtained from patient. Consent for publication: Written informed consent for publication obtained from patient. Competing interests: The authors declare no competing interests.
Figures


References
-
- Fakhouri F, Fremeaux-Bacchi V, Noel LH, Cook HT, Pickering MC. C3 glomerulopathy: a new classification. Nat Rev Nephrol. 2010;6(8):494–9. - PubMed
-
- Fakhouri F, Le Quintrec M, Fremeaux-Bacchi V. Practical management of C3 glomerulopathy and Ig-mediated MPGN: facts and uncertainties. Kidney Int. 2020;98(5):1135–48. - PubMed
-
- Noris M, Daina E, Remuzzi G. Membranoproliferative glomerulonephritis: no longer the same disease and may need very different treatment. Nephrol Dial Transpl. 2023;38(2):283–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
