

The Association of Malignancy With Stroke and Bleeding in Atrial Fibrillation: A Population-Based Cohort Study
- PMID: 39967202
- PMCID: PMC11866432
- DOI: 10.1016/j.jaccao.2024.10.014
The Association of Malignancy With Stroke and Bleeding in Atrial Fibrillation: A Population-Based Cohort Study
Abstract
Background: It is undetermined if malignancy independently increases stroke risk in atrial fibrillation (AF).
Objectives: This study sought to determine the association of malignancy with stroke and bleeding in AF.
Methods: Population-based cohort study using administrative datasets of people aged ≥66 years with newly diagnosed AF. People diagnosed with malignancy within 5 years before AF diagnosis were matched to cancer-free control subjects on age, sex, AF diagnosis details, CHA2DS2-VASc score, and ATRIA bleeding score. Outcomes included hospitalizations for stroke and hospitalization/emergency visits for bleeding. Cause-specific regression was used to determine the HR for malignancy after adjusting for time-varying anticoagulation status. Analyses were repeated for specific subgroups of cancer patients (with matched control subjects).
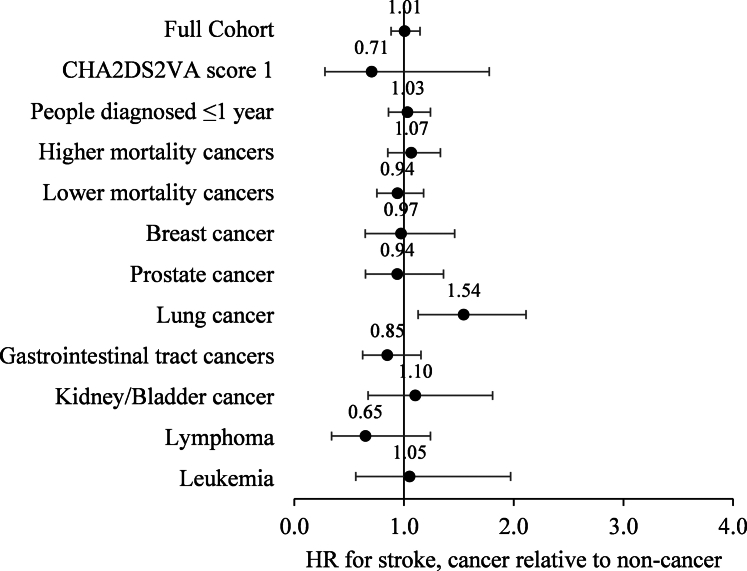
Results: Among 199,710 AF patients, 24,991 (12.5%) people had prior malignancy. Malignancy was associated with more inpatient diagnoses of AF (vs outpatient) and less anticoagulation. We matched 43,802 people with AF (21,901 with malignancy, mean age 78.1 years; 59.5% male). After adjusting for anticoagulation status, malignancy had a similar hazard of stroke (HR: 1.01; 95% CI: 0.88-1.15) but higher hazard of bleeding (HR: 1.45; 95% CI: 1.37-1.53) compared with cancer-free control subjects in the matched sample. Analyses of cancer subgroups with comparison to matched control subjects mostly showed consistent results, except for: 1) increased hazard of stroke in lung cancer; and 2) lack of increased bleeding hazard in breast cancer and lymphoma.
Conclusions: People with AF and malignancy generally had similar hazards of stroke but higher hazards of bleeding compared with cancer-free control subjects, suggesting that malignancy should not lower the threshold for anticoagulation in AF.
Keywords: ATRIA; CHA(2)DS(2)-VASc score; anticoagulation; arrhythmia; atrial fibrillation; bleeding; cancer; cerebrovascular disease; epidemiology; stroke; thrombosis.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was funded by the Canadian Cardiovascular Society Atrial Fibrillation Research Award and the Ted Rogers Program in Cardiotoxicity Prevention. Dr Adam was funded by the Heart & Stroke/Richard Lewar Centre of Excellence in Cardiovascular Research. Dr Abdel-Qadir was supported by a National New Investigator Award from the Heart and Stroke Foundation of Canada. Dr Thavendiranathan was supported by a Tier II Canada Research Chair and the Canadian Cancer Society/Canadian Institutes of Health Research’s W. David Hargraft Grant (no. 706710). This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. This study also received funding from the sources described previously. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. Dr Abdel-Qadir has received consulting and speaker honoraria from Amgen, AstraZeneca, and Jazz Pharmaceuticals. Dr Amir has received honoraria from Seagen, Gilead, Pfizer, and Novartis; and served as a consultant or advisor for AstraZeneca and Novartis. Dr Ha has received speaker honoraria from Bayer, BMS/Pfizer Alliance, and Servier. Dr Thavendiranathan has received consulting and speaker honoraria from GE, Amgen, Boehringer Ingelheim, and AstraZeneca. Dr Fradley has received research grants from Medtronic and AstraZeneca; and consulting fees from AstraZeneca, AbbVie, Janssen, Johnson and Johnson, Pfizer, and Zoll. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
-
- Siegel R.L., Miller K.D., Wagle N.S., Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17–48. - PubMed
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., et al. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147:e93–e621. - PubMed
-
- Hindricks G., Potpara T., Dagres N., et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373–498. - PubMed
-
- Joglar J.A., Chung M.K., Armbruster A.L., et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2024;83(1):109–279. - PMC - PubMed
-
- Farmakis D., Parissis J., Filippatos G. Insights into onco-cardiology: atrial fibrillation in cancer. J Am Coll Cardiol. 2014;63:945–953. - PubMed
LinkOut - more resources
Full Text Sources
