

Quality of life trajectories for different dialysis modalities-a nationwide study
- PMID: 39968507
- PMCID: PMC11833710
- DOI: 10.1093/ckj/sfae420
Quality of life trajectories for different dialysis modalities-a nationwide study
Abstract
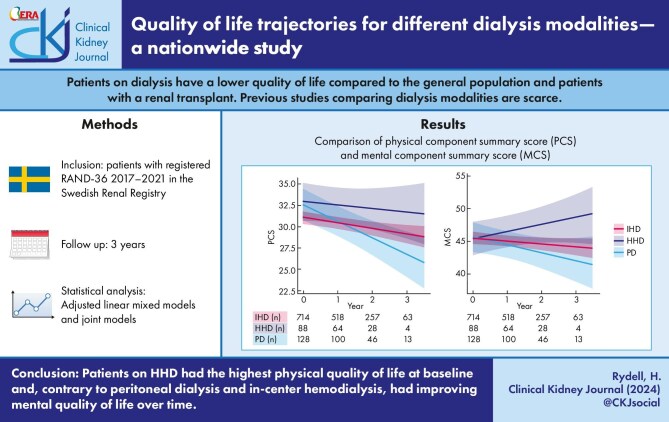
Background: Few contemporary studies have investigated the changes in quality of life across dialysis modalities. Our aim was to compare longitudinal changes in health-related physical and mental quality of life between patients on institutional hemodialysis (IHD), peritoneal dialysis (PD) and home hemodialysis (HHD).
Methods: Patients on dialysis with registered Research and Development 36 (RAND-36) questionnaires between 2017-2021 in the Swedish Renal Registry (SRR) were eligible for inclusion. Information on dialysis, patient characteristics and medication were collected from SRR and other registries. Patients were followed up to 39 months. Changes in physical (PCS) and mental (MCS) component summary scores were analyzed in adjusted linear mixed models and joint models.
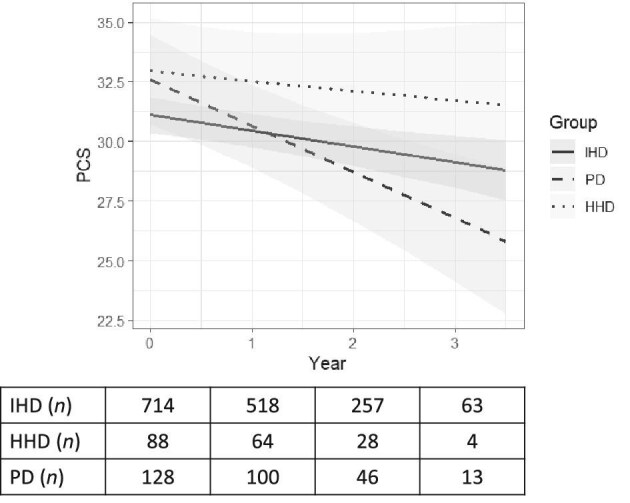
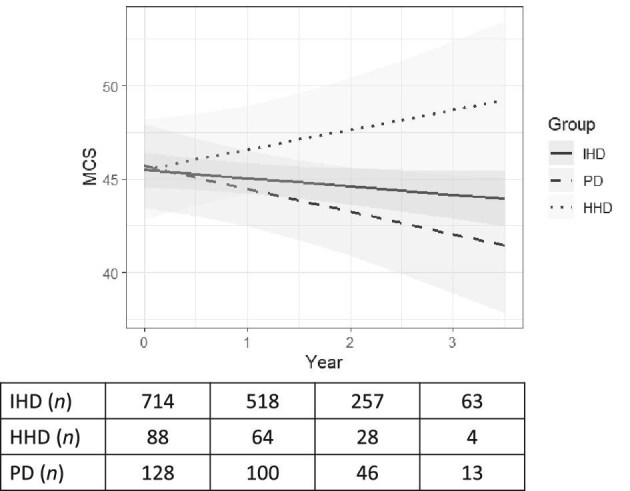
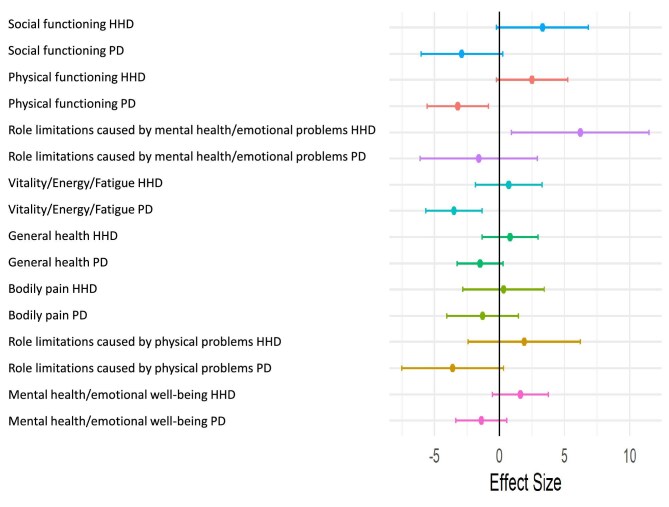
Results: We included 930 patients (IHD 714, PD 128, HHD 88) with a median follow-up of 1.8 years (interquartile range 1.0-2.1). At baseline, the mean unadjusted PCS was lower in IHD (30.7; 95% CI 29.9, 31.4) compared with HHD (35.3; 95% CI 33.0, 37.5) and PD (33.2; 95% CI 31.3, 35.1). PCS declined over time in all modalities, but faster for PD compared with IHD (-1.2; 95% CI -2.1, -0.3 per year) and HHD (-1.5, 95% CI -2.9, -0.04). MCS was similar at baseline. HHD had improving MCS trajectory compared to IHD (-1.5, 95% CI -2.8, 0.2) and PD (-2.3, 95% CI -3.9, 0.7), largely resulting from improvement in role limitations caused by mental health (6.2, 95% CI 0.9, 11.5).
Conclusion: Insights about the variation in quality-of-life trajectories for different dialysis modalities are important for patients to make informed choices.
Keywords: RAND-36; home hemodialysis; in-center hemodialysis; peritoneal dialysis; quality of life.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
M.E., institutional grants from Astellas pharma and Astra Zeneca, payment for lectures and advisory boards from Astellas pharma and Vifor pharma, and payment for lectures from Astra Zeneca, Fresenius Medical Care, and Baxter Healthcare. B.L., previous affiliation with Baxter Healthcare. J.W., payment for lectures from Fresenius Medical Care.
Figures
Similar articles
-
Fewer hospitalizations and prolonged technique survival with home hemodialysis- a matched cohort study from the Swedish Renal Registry.BMC Nephrol. 2019 Dec 30;20(1):480. doi: 10.1186/s12882-019-1644-z. BMC Nephrol. 2019. PMID: 31888674 Free PMC article.
-
Improved long-term survival with home hemodialysis compared with institutional hemodialysis and peritoneal dialysis: a matched cohort study.BMC Nephrol. 2019 Feb 13;20(1):52. doi: 10.1186/s12882-019-1245-x. BMC Nephrol. 2019. PMID: 30760251 Free PMC article.
-
Travel distance and home dialysis rates in the United States.Perit Dial Int. 2014 Jan-Feb;34(1):24-32. doi: 10.3747/pdi.2012.00234. Perit Dial Int. 2014. PMID: 24525595 Free PMC article.
-
A Comparison of Patient-Reported Outcome Measures of Quality of Life By Dialysis Modality in the Treatment of Kidney Failure: A Systematic Review.Can J Kidney Health Dis. 2020 Oct 19;7:2054358120957431. doi: 10.1177/2054358120957431. eCollection 2020. Can J Kidney Health Dis. 2020. PMID: 33149924 Free PMC article. Review.
-
A Systematic Approach To Promoting Home Hemodialysis during End Stage Kidney Disease.Kidney360. 2020 Jul 8;1(9):993-1001. doi: 10.34067/KID.0003132020. eCollection 2020 Sep 24. Kidney360. 2020. PMID: 35369547 Free PMC article. Review.
References
-
- Swedish Renal Registry Annual Report 2022. https://www.medscinet.net/snr/arsrapporter.aspx
LinkOut - more resources
Full Text Sources
