

Non-invasive vagus nerve stimulation and exercise capacity in healthy volunteers: a randomized trial
- PMID: 39969124
- PMCID: PMC7617618
- DOI: 10.1093/eurheartj/ehaf037
Non-invasive vagus nerve stimulation and exercise capacity in healthy volunteers: a randomized trial
Abstract
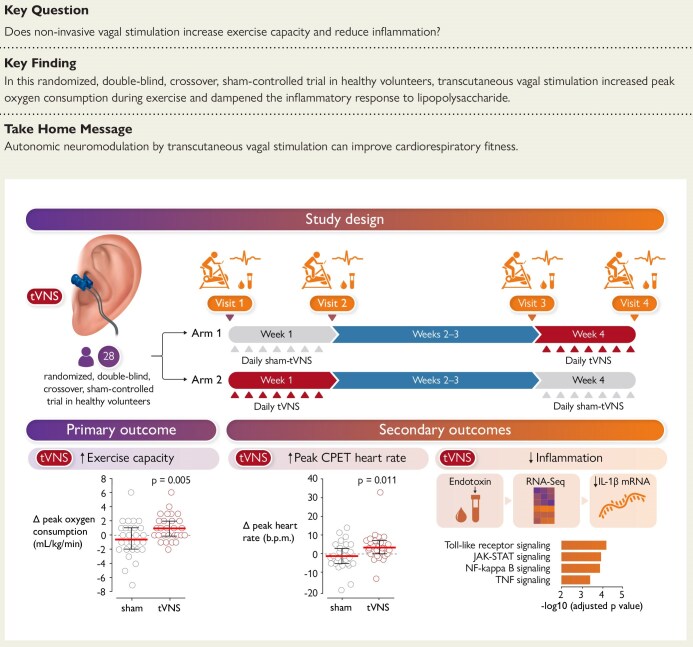
Background and aims: Vagal parasympathetic dysfunction is strongly associated with impaired exercise tolerance, indicating that coordinated autonomic control is essential for optimizing exercise performance. This study tested the hypothesis that autonomic neuromodulation by non-invasive transcutaneous vagus nerve stimulation (tVNS) can improve exercise capacity in humans.
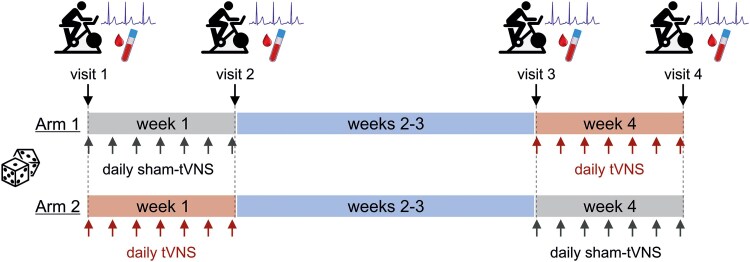
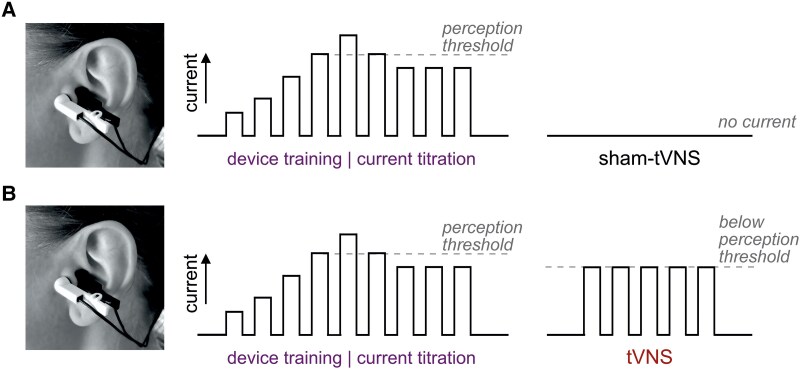
Methods: This single-centre, randomized, double-blind, sham-controlled, crossover trial in 28 healthy volunteers evaluated the effect of bilateral transcutaneous stimulation of vagal auricular innervation, applied for 30 min daily for 7 days, on measures of cardiorespiratory fitness (peak oxygen consumption (VO2peak)) during progressive exercise to exhaustion. Secondary endpoints included peak work rate, cardiorespiratory measures, and the whole blood inflammatory response to lipopolysaccharide ex vivo.
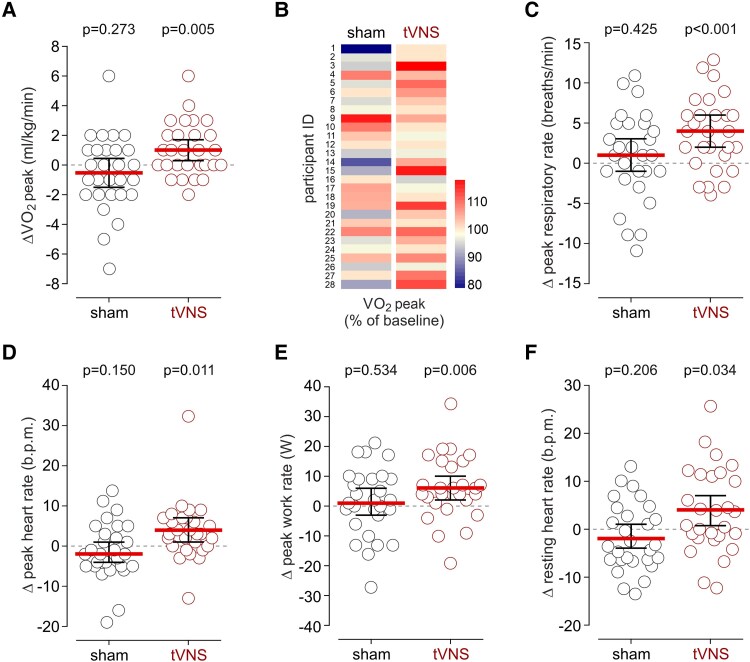
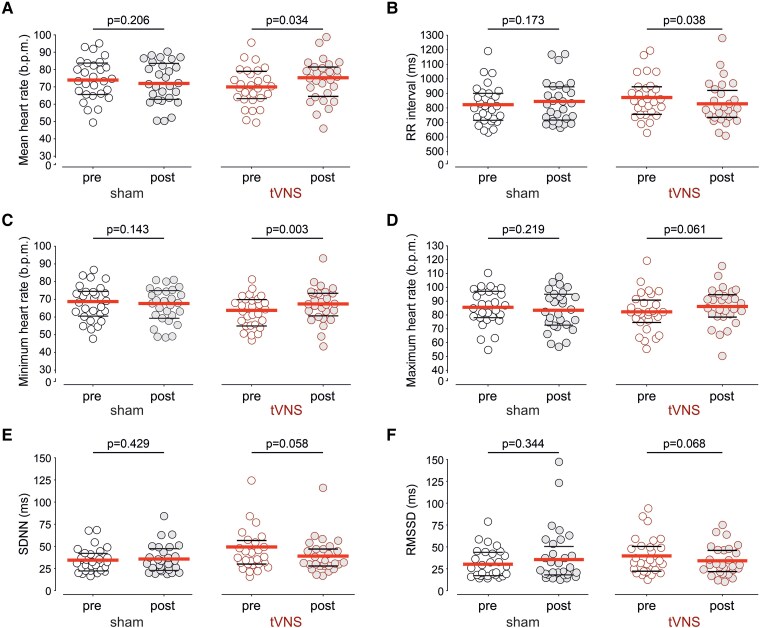
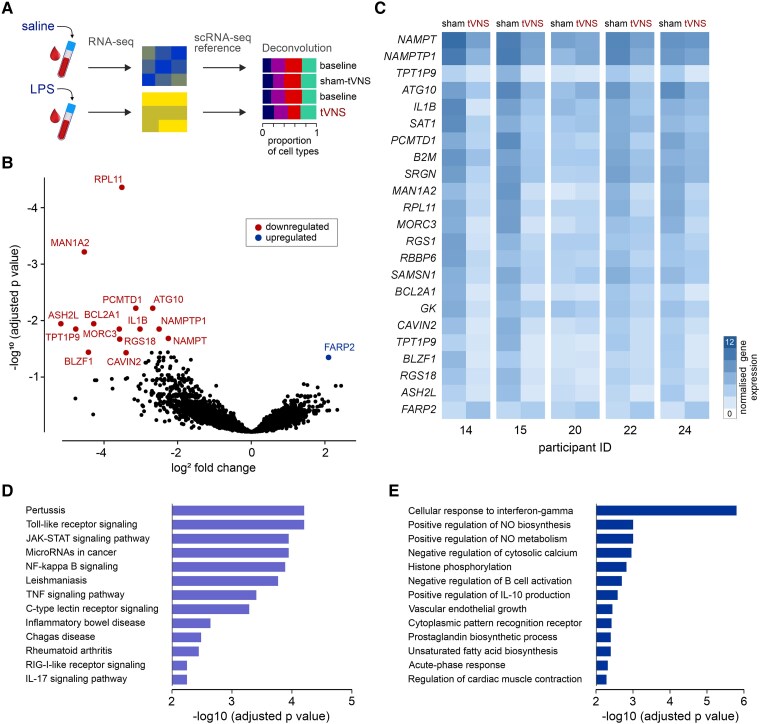
Results: tVNS applied for 30 min daily over 7 consecutive days increased VO2peak by 1.04 mL/kg/min (95% CI: .34-1.73; P = .005), compared with no change after sham stimulation (-0.54 mL/kg/min; 95% CI: -1.52 to .45). No carry-over effect was observed following the 2-week washout period. tVNS increased work rate (by 6 W; 95% CI: 2-10; P = .006), heart rate (by 4 bpm; 95% CI: 1-7; P = .011), and respiratory rate (by 4 breaths/min; 95% CI: 2-6; P < .001) at peak exercise. Analysis of the whole blood transcriptomic response to lipopolysaccharide in serial samples obtained from five participants showed that tVNS reduced the inflammatory response.
Conclusions: Non-invasive vagal stimulation improves measures of cardiorespiratory fitness and attenuates inflammation, offering an inexpensive, safe, and scalable approach to improve exercise capacity.
Keywords: Ageing; Autonomic nervous system; Exercise; Neuromodulation; Vagus nerve.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Similar articles
-
Effects of transcutaneous vagus nerve stimulation in individuals aged 55 years or above: potential benefits of daily stimulation.Aging (Albany NY). 2019 Jul 30;11(14):4836-4857. doi: 10.18632/aging.102074. Aging (Albany NY). 2019. PMID: 31358702 Free PMC article. Clinical Trial.
-
Non-invasive vagus nerve stimulation acutely improves spontaneous cardiac baroreflex sensitivity in healthy young men: A randomized placebo-controlled trial.Brain Stimul. 2017 Sep-Oct;10(5):875-881. doi: 10.1016/j.brs.2017.05.006. Epub 2017 May 19. Brain Stimul. 2017. PMID: 28566194 Clinical Trial.
-
Impact of optimized transcutaneous auricular vagus nerve stimulation on cardiac autonomic profile in healthy subjects and heart failure patients.Physiol Meas. 2024 Jul 17;45(7). doi: 10.1088/1361-6579/ad5ef6. Physiol Meas. 2024. PMID: 39016202 Clinical Trial.
-
Lessons learned from transcutaneous vagus nerve stimulation (tVNS).Epilepsy Res. 2019 Jul;153:83-84. doi: 10.1016/j.eplepsyres.2019.02.015. Epub 2019 Feb 26. Epilepsy Res. 2019. PMID: 30952581 Review.
-
Effects of transcutaneous auricular vagus nerve stimulation on cardiovascular autonomic control in health and disease.Auton Neurosci. 2021 Dec;236:102893. doi: 10.1016/j.autneu.2021.102893. Epub 2021 Oct 9. Auton Neurosci. 2021. PMID: 34649119 Review.
Cited by
-
The vagus nerve: a cornerstone for mental health and performance optimization in recreation and elite sports.Front Psychol. 2025 Jul 11;16:1639866. doi: 10.3389/fpsyg.2025.1639866. eCollection 2025. Front Psychol. 2025. PMID: 40718569 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
