

Respiratory Syncytial Virus Vaccine and Nirsevimab Uptake Among Pregnant People and Their Neonates
- PMID: 39969879
- PMCID: PMC11840647
- DOI: 10.1001/jamanetworkopen.2024.60735
Respiratory Syncytial Virus Vaccine and Nirsevimab Uptake Among Pregnant People and Their Neonates
Abstract
Importance: Two interventions to prevent severe respiratory syncytial virus (RSV) in infants were approved in 2023-a bivalent prenatal RSV prefusion F protein-based (RSVpreF) vaccine and an infant monoclonal antibody (nirsevimab). Understanding their uptake and clinical outcomes is essential for public health planning.
Objective: To describe uptake of the prenatal RSVpreF vaccine and infant nirsevimab.
Design, setting, and participants: This retrospective cohort study was conducted at a single academic center among 647 pregnant individuals eligible for RSVpreF vaccination (32-36 weeks' gestation between October 15, 2023, and January 31, 2024) and infants eligible for nirsevimab (no prenatal RSVpreF vaccination >14 days before delivery).
Exposure: Pregnancy or birth during the 2023-2024 RSV season.
Main outcomes and measures: RSVpreF vaccination among eligible pregnant individuals and nirsevimab administration prior to hospital discharge among eligible infants.
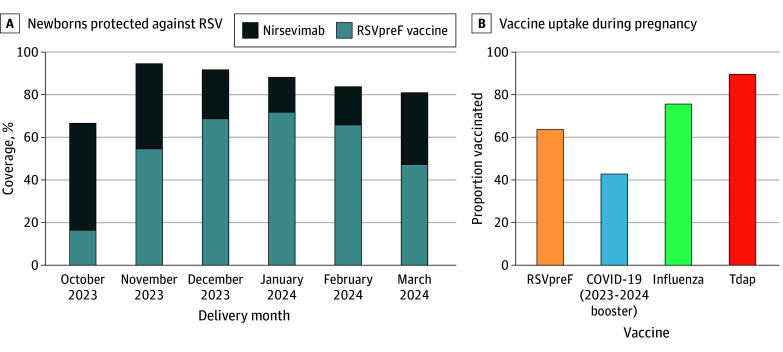
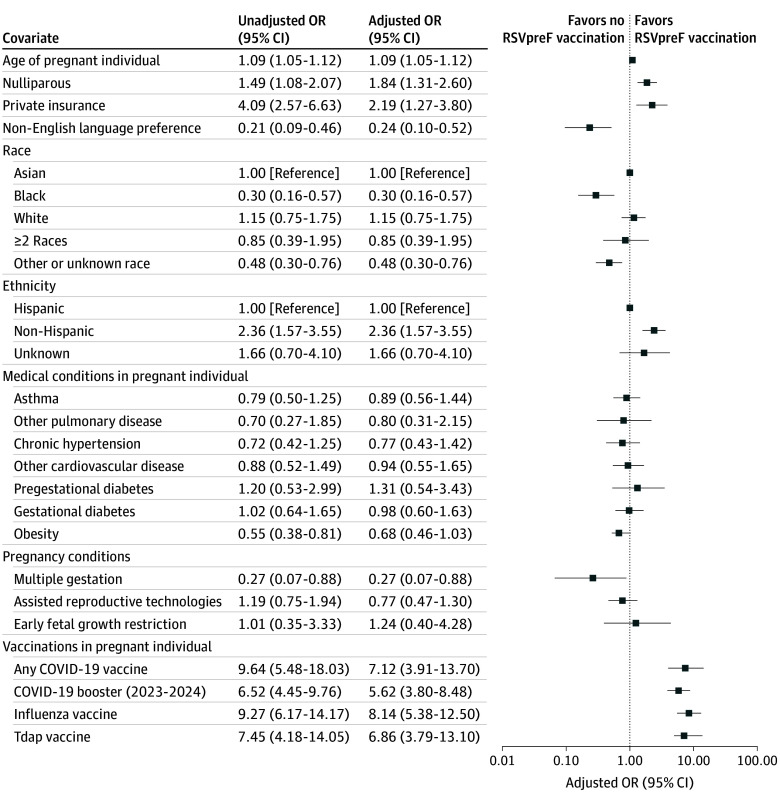
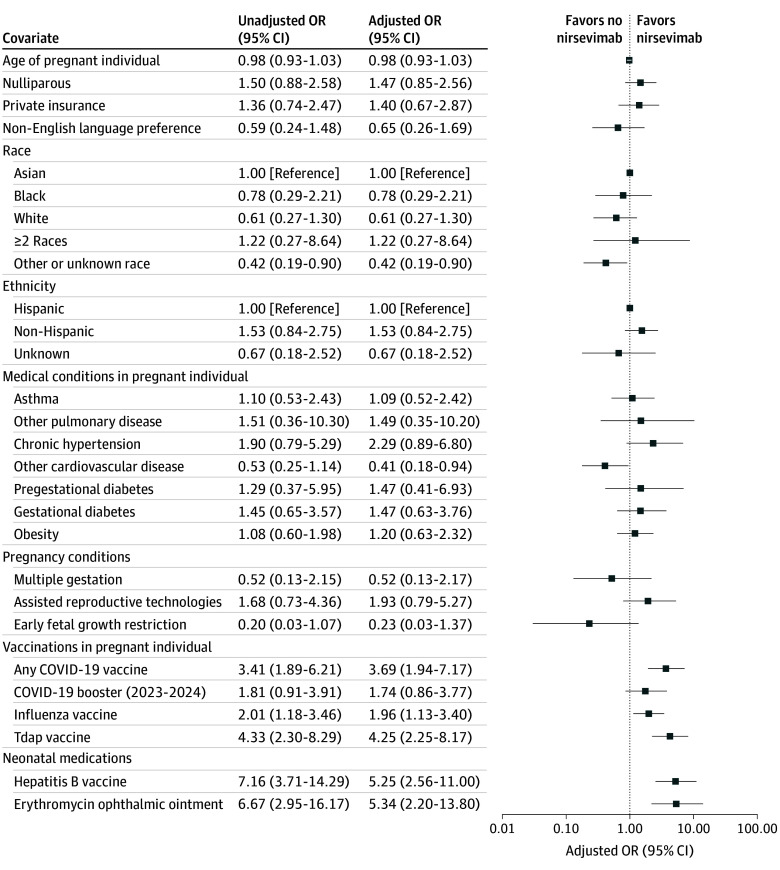
Results: Of 647 eligible pregnant individuals (mean [SD] age, 34.6 [6.2] years; 355 nulliparous [54.9%]; 558 privately insured [86.2%]), 414 (64.0%) received the RSVpreF vaccine. Factors associated with higher RSVpreF uptake included older birthing parent age (adjusted odds ratio [AOR], 1.09; 95% CI, 1.05-1.12), nulliparity (AOR, 1.84; 95% CI, 1.31-2.60), private insurance (AOR, 2.19; 95% CI, 1.27-3.80), non-Hispanic ethnicity (AOR, 2.36; 95% CI 1.57-3.55; reference: Hispanic), receipt of any COVID-19 vaccine (AOR, 7.12; 95% CI, 3.91-13.70), 2023-2024 formula COVID-19 booster vaccine (AOR, 5.62; 95% CI, 3.80-8.48), influenza vaccine (AOR, 8.14; 95% CI, 5.38-12.50), or tetanus-diphtheria-pertussis vaccine (AOR, 6.86; 95% CI, 3.79-13.10). Factors associated with lower RSVpreF uptake included non-English language preference (AOR, 0.24; 95% CI, 0.10-0.52), Black race (AOR, 0.30; 95% CI, 0.16-0.57; reference: Asian), other or unknown race (AOR, 0.48; 95% CI, 0.30-0.76), and multiple gestation (AOR, 0.27; 95% CI, 0.07-0.88). Nirsevimab was administered to 183 of 261 eligible infants (70.1%) prior to hospital discharge. Among those who did not receive RSVpreF or standard prenatal vaccines, 40.4% of their neonates (19 of 47) received nirsevimab; among those who declined infant hepatitis B vaccination, 34.0% of their neonates (17 of 50) received nirsevimab. Respiratory syncytial virus coverage exceeded 80% during all months of the study period except October 2023, the first month during which prenatal RSV vaccination and infant nirsevimab were available. Preterm delivery occurred in 35 of 414 RSVpreF-vaccinated individuals (8.5%) and 43 of 233 unvaccinated individuals (18.5%). In a nested case-control analysis with preterm birth as the outcome, there was no significant association between RSVpreF vaccination and preterm birth (AOR, 1.03; 95% CI, 0.55-1.93).
Conclusions and relevance: In this cohort study, uptake of the RSVpreF vaccine and infant nirsevimab was high. Nirsevimab uptake was high even among individuals who did not receive routine prenatal or infant vaccines. There was no significant association between RSVpreF vaccination and preterm birth. This study suggests that an RSV prevention strategy that included both prenatal vaccination and infant monoclonal antibody administration had high uptake and reassuring perinatal outcomes.
Conflict of interest statement
Figures
Comment in
References
-
- Shi T, McAllister DA, O’Brien KL, et al. ; RSV Global Epidemiology Network . Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946-958. doi:10.1016/S0140-6736(17)30938-8 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
