

Lessons learned from a candidate gene study investigating aromatase inhibitor treatment outcome in breast cancer
- PMID: 39971965
- PMCID: PMC11840073
- DOI: 10.1038/s41523-025-00733-y
Lessons learned from a candidate gene study investigating aromatase inhibitor treatment outcome in breast cancer
Abstract
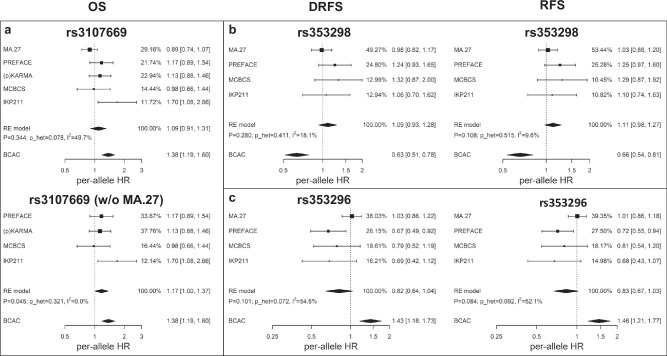
The role of germline genetics in adjuvant aromatase inhibitor (AI) treatment efficacy in ER-positive breast cancer is poorly understood. We employed a two-stage candidate gene approach to examine associations between survival endpoints and common germline variants in 753 endocrine resistance-related genes. For a discovery cohort, we screened the Breast Cancer Association Consortium database (n ≥ 90,000 cases) and retrieved 2789 AI-treated patients. Cox model-based analysis revealed 125 variants associated with overall, distant relapse-free, and relapse-free survival (p-value ≤ 1E-04). In validation analysis using five independent cohorts (n = 8857), none of the six selected candidates representing major linkage blocks at CELA2B/CASP9, NR1I2/GSK3B, LRP1B, and MIR143HG (CARMN) were validated. We discuss potential reasons for the failed validation and replication of published findings, including study/treatment heterogeneity and other limitations inherent to genomic treatment outcome studies. For the future, we envision prospective longitudinal studies with sufficiently long follow-up and endpoints that reflect the dynamic nature of endocrine resistance.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Peter A. Fasching reports personal fees from Novartis, Pfizer, Daiichi-Sankyo, AstraZeneca, Eisai, Merck Sharp & Dohme, Lilly, Pierre Fabre, SeaGen, Roche, Hexal, Agendia, and Gilead and grants from Biontech and Cepheid. Carolin C. Hack received Honoraria from AstraZeneca, Daiichi Sankyo, Eisai, Novartis, Pfizer, Roche, Gilead and MSD as well as support for attending meetings from Daiichi Sankyo. Matthias Schwab received funding from Agena Bioscience GmbH, HepaRegenix GmbH, Robert Bosch GmbH, and CORAT Therapeutics GmbH, as well as honoraria for oral presentations at academically organized congresses and meetings; he received payment for expert testimony from the Research Impact Fund Committee (RIF), Research Grant Council (RCG), Hong Kong, and from the German Federal Ministry of Education and Research (BMBF); he is (section-) editor for Pharmacogenetics and Genomics, Drug Research, and Genome Medicine. Diana M. Eccles has received research support from AstraZeneca. Matthew P. Goetz reports consulting fees to Mayo Clinic from ARC Therapeutics, AstraZeneca, Biotheranostics, Blueprint Medicines, Lilly, Novartis, Rna Diagnostics, Sanofi Genzyme, Seattle Genetics, Sermonix, Engage Health Media, Laekna and TerSera Therapeutics/Ampity Health; grant funding to Mayo Clinic from Lilly, Pfizer, Sermonix, Loxo, AstraZeneca and ATOSSA Therapeutics; personal fees for CME activities from Research to Practice, Clinical Education Alliance, Medscape, and MJH Life Sciences; personal fees serving as a panelist for a panel discussion from Total Health Conferencing and personal fees for serving as a moderator for Curio Science; and travel support from Lilly. All other authors report no conflict of interest.
Figures


References
-
- Sung, H. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin.71, 209–249 (2021). - PubMed
-
- Smith, I. E. & Dowsett, M. Aromatase inhibitors in breast cancer. N. Engl. J. Med.348, 2431–2442 (2003). - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials. Lancet386, 1341–1352 (2015). - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in premenopausal women with oestrogen receptor-positive early-stage breast cancer treated with ovarian suppression: a patient-level meta-analysis of 7030 women from four randomised trials. Lancet Oncol. 23, 382–392 (2022). - PMC - PubMed
Grants and funding
- U19 GM061388/GM/NIGMS NIH HHS/United States
- 01KW0114/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- 110828/Deutsche Krebshilfe (German Cancer Aid)
- U10 CA077202/CA/NCI NIH HHS/United States
- 01KW9976/8/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- C1275/A15956/Cancer Research UK (CRUK)
- 2013PR044/Breast Cancer Campaign/United Kingdom
- C12292/A11174/Cancer Research UK (CRUK)
- NMRC/CIRG/1423/2015/MOH | National Medical Research Council (NMRC)
- C5047/A15007/Cancer Research UK (CRUK)
- C1275/A11699/Cancer Research UK (CRUK)
- R01 CA192393/CA/NCI NIH HHS/United States
- R01 CA196648/CA/NCI NIH HHS/United States
- HEALTH-F2-2009-223175/EC | EC Seventh Framework Programm | FP7 Health (FP7-HEALTH - Specific Programme "Cooperation": Health)
- BMBF 01ZP0502/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- 2010PR62/Breast Cancer Campaign/United Kingdom
- 01KW9977/0/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- R01 CA176785/CA/NCI NIH HHS/United States
- 01KH040/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- DFG Do761/15-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- C5047/A8384/Cancer Research UK (CRUK)
- PPRPGM-Nov20\100002/Cancer Research UK (CRUK)
- EXC 2180-390900677/Deutsche Forschungsgemeinschaft (German Research Foundation)
- 110826/Deutsche Krebshilfe (German Cancer Aid)
- CCS 015469/Canadian Cancer Society Research Institute (Société Canadienne du Cancer)
- 01KW9975/5/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- 106332/Deutsche Krebshilfe (German Cancer Aid)
- C8197/A16565/Cancer Research UK (CRUK)
- C1287/A10710/Cancer Research UK (CRUK)
- C1287/A10118/Cancer Research UK (CRUK)
- R01 CA128978/CA/NCI NIH HHS/United States
- U19 CA148537/CA/NCI NIH HHS/United States
- C1275/A19187/Cancer Research UK (CRUK)
- R01 CA116167/CA/NCI NIH HHS/United States
- 70-2892-BR I/Deutsche Krebshilfe (German Cancer Aid)
- P50 CA116201/CA/NCI NIH HHS/United States
- MOH-000377/MOH | National Medical Research Council (NMRC)
- C1287/A16563/Cancer Research UK (CRUK)
- C5047/A10692/Cancer Research UK (CRUK)
- U01 CA164920/CA/NCI NIH HHS/United States
- R35 CA253187/CA/NCI NIH HHS/United States
- 108419/Deutsche Krebshilfe (German Cancer Aid)
- U19 CA148112/CA/NCI NIH HHS/United States
- U19 CA148065/CA/NCI NIH HHS/United States
- SCHR 1323/2-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- 108253/Deutsche Krebshilfe (German Cancer Aid)
- C1275/C22524/Cancer Research UK (CRUK)
- C1281/A12014/Cancer Research UK (CRUK)
- MOH-000984/MOH | National Medical Research Council (NMRC)
LinkOut - more resources
Full Text Sources
Miscellaneous
