

Atezolizumab following definitive chemoradiotherapy in patients with unresectable locally advanced esophageal squamous cell carcinoma - a multicenter phase 2 trial (EPOC1802)
- PMID: 39972105
- PMCID: PMC11949839
- DOI: 10.1038/s43018-025-00918-1
Atezolizumab following definitive chemoradiotherapy in patients with unresectable locally advanced esophageal squamous cell carcinoma - a multicenter phase 2 trial (EPOC1802)
Abstract
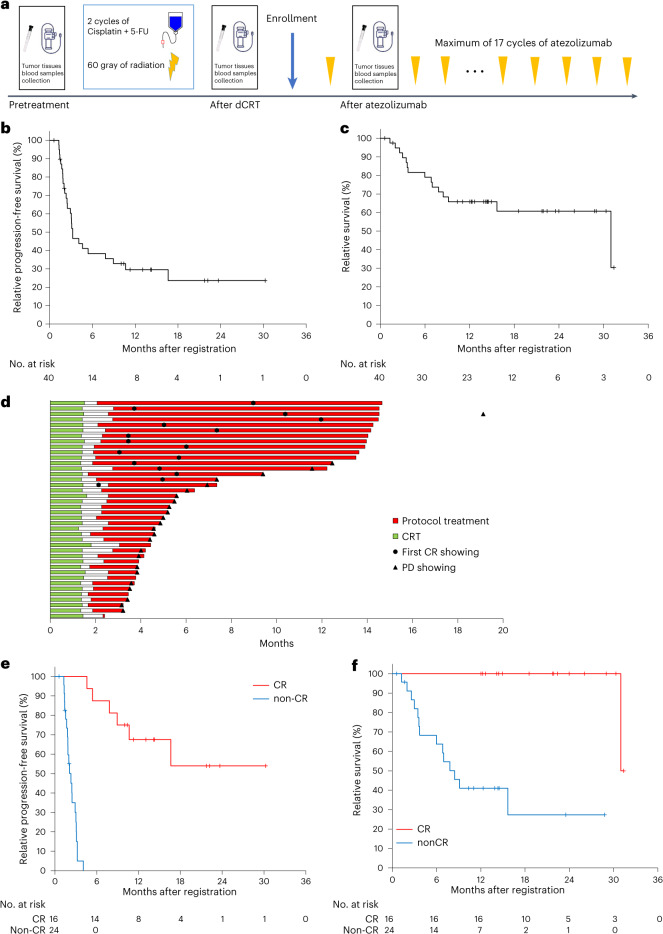
Platinum-based definitive chemoradiotherapy (dCRT) is the standard treatment for patients with unresectable locally advanced esophageal squamous cell carcinoma (ESCC) that invades the aorta, vertebral body or trachea; however, complete response rates remain low (11-25%), leading to poor survival. To evaluate the additive efficacy of the anti-PD-L1 antibody drug atezolizumab, we conducted a phase 2, multicenter, single-arm trial of 1 year of atezolizumab treatment following dCRT in 40 patients with unresectable locally advanced ESCC recruited from seven Japanese centers (UMIN000034373). The confirmed complete response (cCR) rate (primary end point) of the first consecutive 38 patients was 42.1% (90% CI 28.5-56.7%). Regarding the secondary end points, the median progression-free survival and 12-month progression-free survival rates of all 40 patients were 3.2 months and 29.6%, respectively, and the preliminary median overall survival with short-term follow-up and 12-month overall survival rate were 31.0 months and 65.8%, respectively. Other secondary end points evaluated included the cCR rate determined by an investigator's assessment in the locoregionally recurrent ESCC cohort, cCR rate determined by central assessment, overall response rate and incidence of adverse events. No treatment-related death occurred during the study. Atezolizumab monotherapy after dCRT resulted in a promising cCR rate, although long-term survival data are required.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: H.B. reports research funding from Ono Pharmaceutical and honoraria from Ono Pharmaceutical, Eli Lilly Japan and Taiho Pharmaceutical. S. Kumagai received honoraria from MSD and Chugai Pharmaceutical. S.M. received honoraria from Eli Lilly, Merck Biopharma and Chugai Pharmaceutical. K.I. received honoraria from MSD and Chugai Pharmaceutical. T.T. received honoraria from Ono Pharmaceutical, Bristol Myers Squibb, MSD and Taiho Pharmaceuticals. H. Hara reported honoraria from Asahi-Kasei, Bayer, Bristol Myers Squibb, Chugai, Daiichi Sankyo, Lilly, Merck Biopharma, MSD, Ono, Taiho, Takeda and Yakult; consulting or advisory roles from Bristol Myers Squibb, Boehringer Ingelheim, Daiichi Sankyo and Ono; and research grants from ALX Oncology, Amgen, Astellas, AstraZeneca, Bayer, BeiGene, Boehringer Ingelheim, Bristol Myers Squibb, Chugai, Daiichi Sankyo, Eisai, Janssen, MSD, Ono and Taiho. S. Kadowaki reports grants from Ono Pharmaceutical, Taiho Pharmaceutical, MSD, Nobel Pharmaceutical, Janssen Pharmaceutical, Bayer, Eli Lilly, Chugai Pharmaceutical and Daiichi Sankyo, and honoraria from Ono Pharmaceutical, Taiho Pharmaceutical, MSD, Daiichi Sankyo, Merck KgaA, Bristol Myers Squibb, Eli Lilly, Chugai Pharmaceutical, Bayer and Esai. K.K. reports consulting fees from Ono Pharmaceutical, Bristol Myers Squibb, Beigene/Novartis, AstraZeneca, Roche, BAYER, Merck & Co., Merck Biopharma and Janssen; and honoraria from Ono Pharmaceutical and Bristol Myers Squibb. K.C. received grants from Bristol Myers Squibb and Ono for this study and honoraria from Bristol Myers Squibb, Chugai, Ono and Taiho outside of the submitted work. M.N. received personal fees from AstraZeneca, MSD, Varian Medical Systems and Illumina outside the submitted work. M.W. reports honoraria from Nihon Media Physics. S. Koyama reports receiving research funding from Otsuka Pharmaceutical and Chugai Pharmaceutical. H.M. received research funding from Ono Pharmaceutical, PFDeNA, Konica-Minolta, Ambry Genetics, Chugai, Guardant Health and Riken Genesis outside this study; and also serves as a board member of CureGene outside this study. H.N. received research funding and honoraria (lecture fees) from Ono Pharmaceutical, Bristol Myers Squibb, Chugai Pharmaceutical and MSD; honoraria (lecture fees) from Amgen; and research funding from Taiho Pharmaceutical, Daiichi Sankyo, Kyowa Kirin, Zenyaku Kogyo, Oncolys BioPharma, Debiopharma, Asahi-Kasei, Sysmex, Fujifilm, SRL, Astellas Pharmaceutical, Sumitomo Dainippon Pharma and BD Japan outside this study. He also serves as a board member and founder of Sustainable Cell Therapeutics and Cellian-Biclo outside this study. K.S. reports receiving personal fees for advisory roles from Lilly, Bristol Myers Squibb, Takeda, Pfizer, Ono Pharmaceutical, Merck Pharmaceutical, Taiho Pharmaceutical, Astellas, Novartis, AbbVie, GSK, Daiichi Sankyo, Amgen, Boehringer Ingelheim, Guardant Health Japan and Janssen; receiving honoraria (lecture fees) from Takeda, Bristol Myers Squibb and Janssen; and receiving research funding from Astellas, Ono Pharmaceutical, Daiichi Sankyo, Taiho Pharmaceutical, Chugai, Merck Pharmaceutical, Medi Science, Eisai and Amgen, outside the submitted work. T.Y. reports research funding from Taiho, Ono, Chugai, Amgen, MSD, Daiichi Sankyo, Eisai, FALCO Biosystems, Genomedia, Molecular Health, Nippon Boehringer Ingelheim, Pfizer, Roche Diagnostics, Sysmex and Sanofi and honoraria from Bayer, Chugai, Merck Biopharma, MSD, Ono and Takeda. T.K. reports honoraria from Ono Pharmaceutical, Covidien Japan, MSD, Boehringer Ingelheim, Kyowa Kirin, EA Pharma, Bristol Myers Squibb, 3H Clinical Trial, AstraZeneca, Taiho Pharmaceutical, LiangYiHui Healthcare, Oncology News China, Japanese Society of Pharmaceutical Health Care and Sciences, Oncolys BioPharma and BMS; and research grants from Beigene Ltd., AstraZeneca, Chugai Pharmaceutical, Parexel International, Shionogi, Taiho Pharmaceutical, Astellas Amgen BioPharma, MSD and Ono Pharmaceutical. The other authors declare no competing interests.
Figures










References
-
- Sung, H. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.71, 209–249 (2021). - PubMed
-
- Obermannova, R. et al. Oesophageal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol.33, 992–1004 (2022). - PubMed
-
- Ajani, J. A. et al. Esophageal and esophagogastric junction cancers, Version 2.2023, NCCN Clinical Practice Guidelines in Oncology. J. Natl Compr. Canc. Netw.10.6004/jnccn.2023.0019 (2023). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
