

EIT guided evaluation of regional ventilation distributions in neonatal and pediatric ARDS: a prospective feasibility study
- PMID: 39972380
- PMCID: PMC11841312
- DOI: 10.1186/s12931-025-03134-8
EIT guided evaluation of regional ventilation distributions in neonatal and pediatric ARDS: a prospective feasibility study
Erratum in
-
Correction: EIT guided evaluation of regional ventilation distributions in neonatal and pediatric ARDS: a prospective feasibility study.Respir Res. 2025 Jun 4;26(1):208. doi: 10.1186/s12931-025-03292-9. Respir Res. 2025. PMID: 40468296 Free PMC article. No abstract available.
Abstract
Background: Despite international guidelines for lung protective ventilation in neonatal or pediatric acute respiratory distress syndrome (nARDS/ pARDS), prospective data on bedside monitoring tools for regional ventilation distribution and lung mechanics are still rare. As a bedside and radiation-free procedure, electrical impedance tomography (EIT) offers a practical and safe approach for analyzing regional ventilation distributions. Recent trials in adults have shown the efficacy of an individualized EIT guided strategy for the improvement of ventilator induced lung injury (VILI).
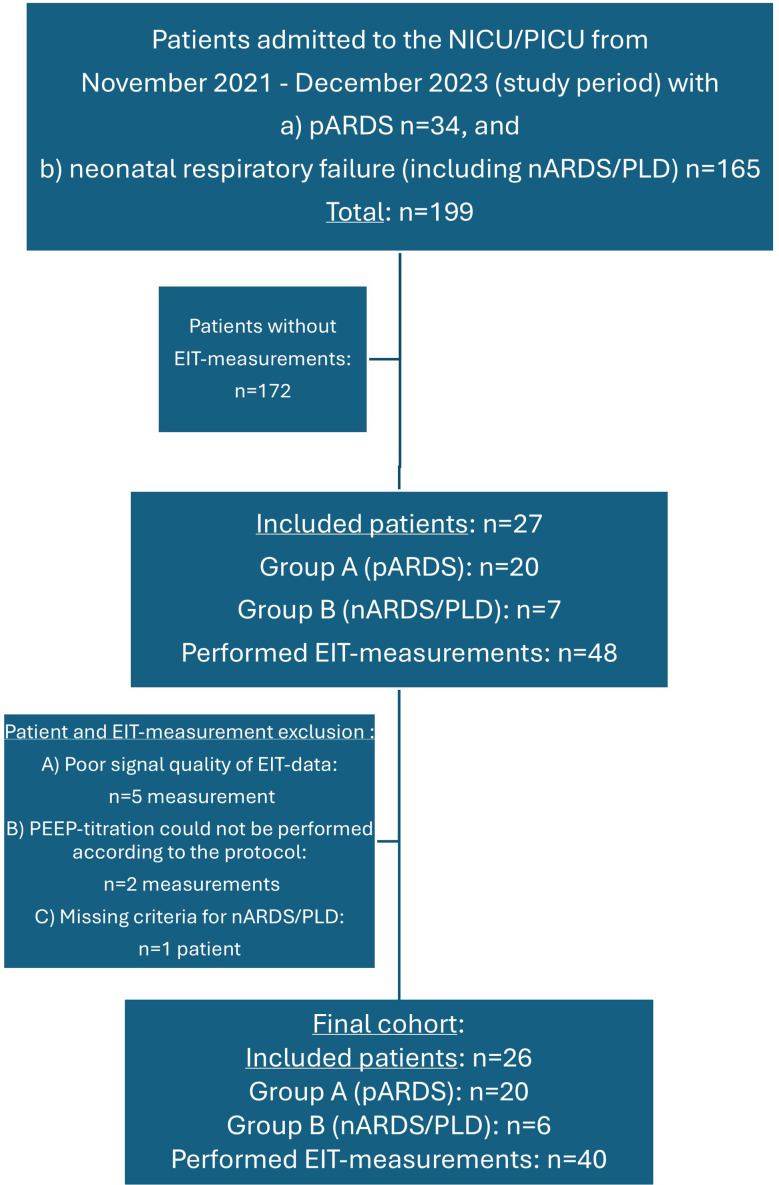
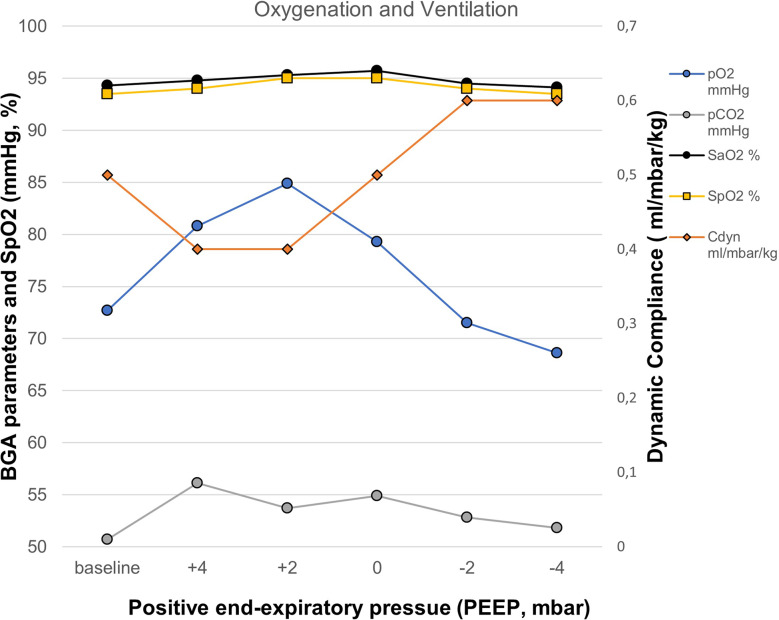
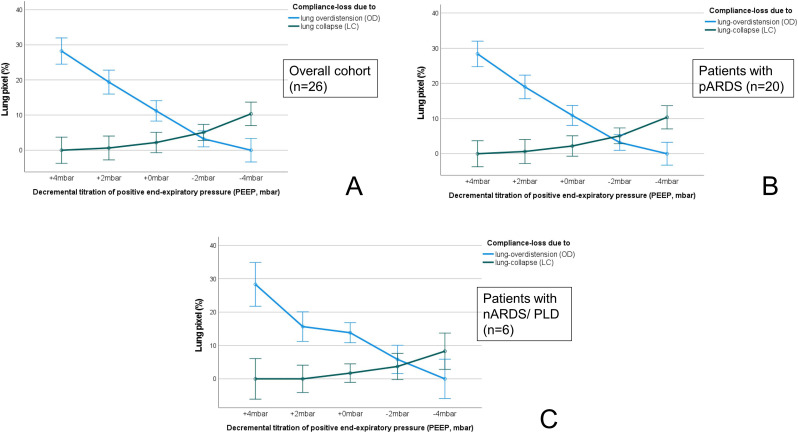
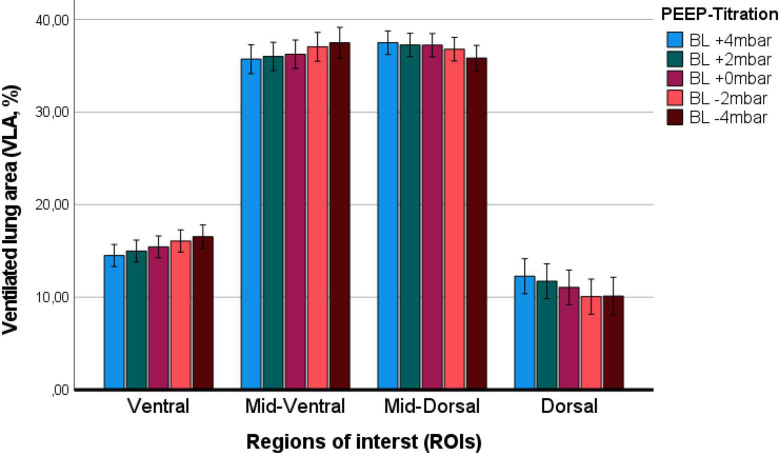
Methods: We performed a single-center prospective feasibility study from November/2021 to December/2023 in the department of neonatal and pediatric intensive care medicine at the University Children´s Hospital in Bonn. All patients with diagnosis of nARDS (or history of perinatal lung disease-PLD)/ pARDS were screened for study inclusion. In all patients a decremental PEEP (positive end-expiratory pressure) trial was performed with a continuous EIT monitoring for an individual analysis of the EIT guided pixel compliance (CEIT) and PEEP finding (EIT-PEEP). In the offline analysis, further EIT derived indices, such as global inhomogeneity index (GI), and center of ventilation (CoV), were calculated.
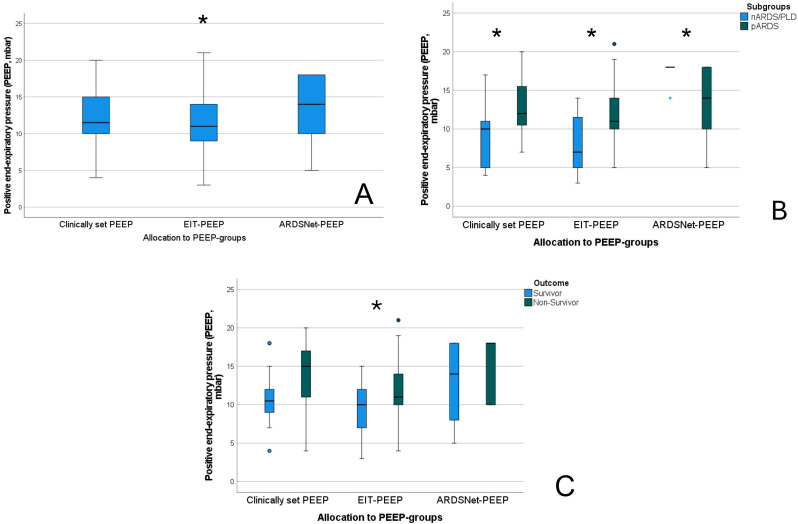
Results: Overall, 40 EIT measurements were performed in 26 neonatal and pediatric patients (nARDS/PLD, n = 6; and pARDS, n = 20) within a predefined decremental PEEP trial. Thirteen patients were classified as having severe nARDS (PLD)/ pARDS with an Oxygen Saturation Index (OSI) > 12 or Oxygenation Index (OI) > 16. In-hospital mortality rate was 27% in the overall cohort. The median EIT-PEEP (11mbar) was calculated as lowest, as compared to the clinically set PEEP (11.5mbar, p < 0.001), and the ARDSnetwork PEEP table recommendation (ARDSnet-PEEP, 14mbar, p = 0.018). In patients with nARDS/PLD, the EIT-PEEP was calculated 3mbar below the clinically set PEEP (p = 0.058) and 11 mbar below the ARDSnet-PEEP (p = 0.01). In the linear regression analysis, EIT-PEEP and the dynamic compliance (CDYN) at -2mbar presented a significant correlation with a Cohen´s R2 of 0.265 (β: 0.886, p = 0.005).
Conclusion: EIT is feasible and can be performed safely in patients with diagnosis of nARDS/PLD and pARDS, even during ongoing extracorporeal membrane oxygenation (ECMO) support. An individualized PEEP finding strategy according to the EIT compliance might optimize regional ventilation distribution in these patients and can potentially decrease VILI.
Clinical trial registration: The study was registered at the German Clinical Trials Register (GCT; trial number: DRKS 00034905, Registration Date 15.08.2024). The registration was performed retrospectively after inclusion of the last patient.
Keywords: Acute respiratory distress syndrome; Electrical impedance tomography; Neonatal; Pediatric; Regional ventilation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: was given by the Institutional Review Board of the Medical Center of the University of Bonn (local running number 048/21) and the study was conducted according to the declaration of Helsinki. The study was registered at the German Clinical Trials Register (GCT; trial number: DRKS 00034905, Registration Date 15.08.2024). The registration was performed retrospectively after inclusion of the last patient. Patient consent: Patients were prospectively enrolled in the study after informed written consent was obtained from the parents or legal representative. Consent for publication: In our study no images with identification of study participants (patients) or health care workers (attending physician or nursing stuff) can be identified. Therefore, we there was no need to obtain written consent for publication purposes prior to manuscript submission. Competing interests: The authors declare no competing interests.
Figures

References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342:1334–49. 10.1056/NEJM200005043421806. PubMed PMID: 10793167. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
