

Multimodality Imaging Findings in Cardiac Plasmacytoma
- PMID: 39972692
- PMCID: PMC11861942
- DOI: 10.1016/j.jaccas.2024.102605
Multimodality Imaging Findings in Cardiac Plasmacytoma
Abstract
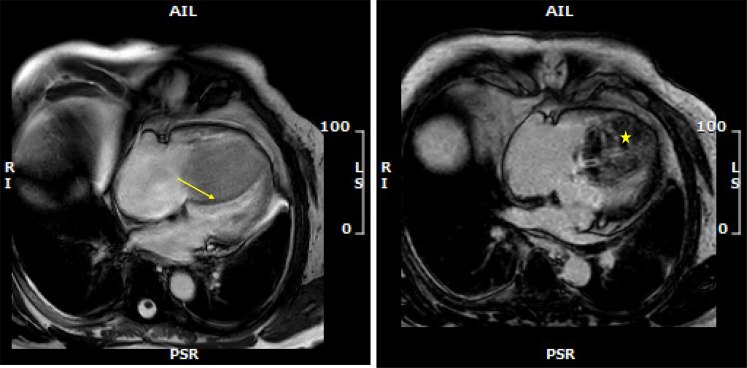
Extramedullary plasmacytoma involving the heart is a rare occurrence. We present the case of a 74-year-old man who received a diagnosis of cardiac plasmacytoma in the context of relapsed multiple myeloma. The tumor primarily presented as a solitary extramedullary plasmacytoma with extensive infiltration into the right ventricle, leading to mild symptoms such as dyspnea. There was no evidence of systemic involvement. A treatment with DRd (daratumumab, lenalidomide, and dexamethasone) was promptly initiated. This case demonstrates the effective use of multimodal imaging techniques to characterize cardiac masses and to determine the most appropriate management plan.
Keywords: cardiac magnetic resonance; computed tomography; echocardiography; heart; plasmacytoma; positron emission tomography-computed tomography.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures









References
-
- Reynen K. Frequency of primary tumors of the heart. Am J Cardiol. 1996;77:107. - PubMed
-
- Tazelaar H.D., Locke T.J., McGregor C.G. Pathology of surgically excised primary cardiac tumors. Mayo Clin Proc. 1992;67:957–965. - PubMed
-
- Molina J.E., Edwards J.E., Ward H.B. Primary cardiac tumors: experience at the University of Minnesota. Thorac Cardiovasc Surg. 1990;38(suppl 2):183–191. - PubMed
-
- Sequist L.V., Han J.Y., Ahn M.J., et al. Osimertinib plus savolitinib in patients with EGFR mutation-positive, MET-amplified, non-small-cell lung cancer after progression on EGFR tyrosine kinase inhibitors: interim results from a multicentre, open-label, phase 1b study. Lancet Oncol. 2020;21:373–386. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
